
Does Methadone Help Reduce Recidivism?
Methadone is an evidence-based medication for the treatment of opioid use disorder. Some jails and prisons, however, do not allow inmates to remain on this medication as they do medications for psychiatric and other health conditions. What happens when inmates are allowed to remain on methadone – does it make a difference?
WHAT PROBLEM DOES THIS STUDY ADDRESS?
For individuals in the criminal justice system, half meet criteria for a drug use disorder based on the diagnostic and statistical manual of mental disorders (DSM), a substantially higher rate than in the general population. Importantly, as highlighted in prior Recovery Research Institute bulletins, taking medications for opioid use disorder, such as buprenorphine (Suboxone, an opioid agonist that partially stimulates the opioid receptors to help reduce craving and maintain opioid tolerance) or naltrexone (an opioid antagonist that blocks the opioid receptors to help reduce craving), are related to improved opioid outcomes including reduced risk of overdose for incarcerated individuals).
Also, however, it is common practice for jail/prison staff to mandate and facilitate opioid detoxification for individuals who present on methadone, which was long the gold standard of medication for opioid use disorder given studies showing it can help reduce opioid use and improve other health related outcomes (e.g., reduce injection use and incidence of Hepatitis C and HIV). As has been documented across several media outlets, opioid overdose rates have spiked during the last several years.
One common risk factor for overdose occurs when individuals are incarcerated. If prisons force individuals to enter opioid detoxification, this reduces their tolerance to opioids. Then upon release, if they use an amount similar to the amount they used when they were using more regularly and their tolerance was higher, they are vulnerable to overdose because the brain is no longer accustomed to that level of opioid. In this study, Westerberg and colleagues conducted a program evaluation in one criminal justice setting, to investigate whether allowing individuals who were already on methadone, to remain on methadone while incarcerated, in order to reduce rates of re-arrest (i.e., recidivism).
HOW WAS THIS STUDY CONDUCTED?
Authors used a retrospective, naturalistic design to examine outcomes of 118 individuals who were on methadone in the community and then were able to remain on methadone while in jail, in comparison to three other groups of inmates:
- 237 individuals who received opioid detoxification when entering jail
- 220 individuals who received alcohol detoxification
- 385 individuals with no apparent history of substance use disorder.
(It is worth noting that jail is a criminal justice setting for individuals who may be awaiting trial, or whose sentence is generally less than 1 year if they have already had a trial. This is in contrast with “prison”, a setting for individuals whose sentence is generally for 1 or more years.)
In order to create the three comparison groups, authors randomly selected 20% of the 14,962 inmates who were released during the same six-month period as the inmates allowed to remain on methadone. If a randomly selected individual had the necessary characteristics to be placed in one of the comparison groups, they were included in the study. The on-premises methadone program included coordination with the inmates “home clinic” to verify community methadone participation and to determine medication dose. The program also included “as much cognitive-behavioral counseling as the duration of incarceration allowed”, though the specific counseling dose was unclear. After release, staff from the jail methadone program helped coordinate re-engagement with the individual’s community program.
The four groups were compared on two primary study outcomes:
- Likelihood of re-arrest (yes or no)
- Number of days until they were re-arrested, up to 1 year after their release
- If individuals had not been re-arrested by the 1-year cut-point, days to re-arrest were counted as 366 in analyses
The study participants were 50% Hispanic/Latino, 26% White, 15% Native American, and 6% Black. About one-fourth (26%) were female. They were incarcerated, on average, for 53 days prior to release. Because individuals cannot be randomly assigned to naturalistically formed groups, it is particularly important to see if there were differences between these groups of individuals at the outset as such differences also could account for any observed differences in re-arrest rates. Indeed, Native Americans were more likely to be in the alcohol detoxification group than the other groups, the methadone and opioid detoxification group had more Hispanic/Latino individuals than the other two groups, and the general population group had more White individuals than the full sample. The methadone and general population groups had longer jail stays than each of the other two groups. The reasons for these differences are not clear but are important to note in understanding and contextualizing any findings where there are group differences on the two primary outcomes mentioned earlier.
WHAT DID THIS STUDY FIND?
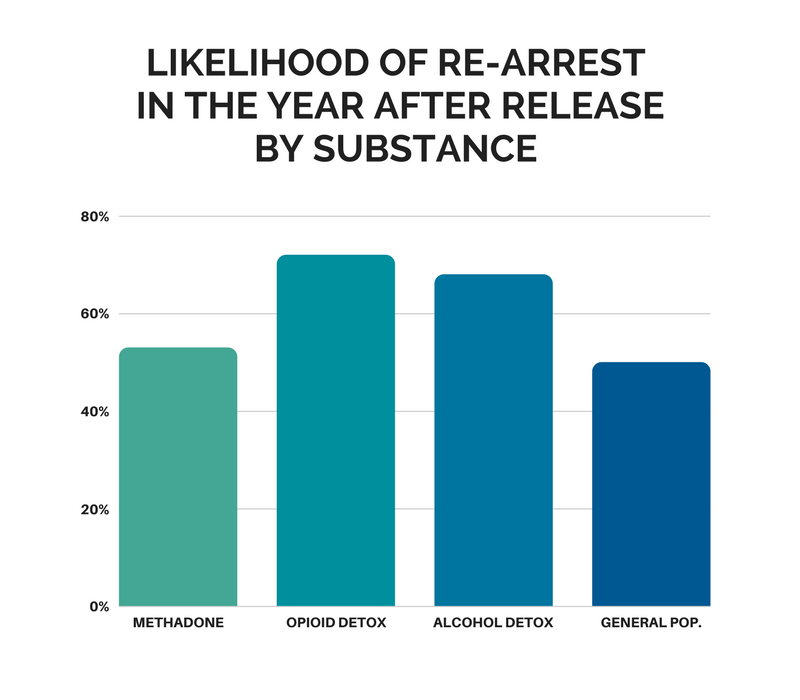
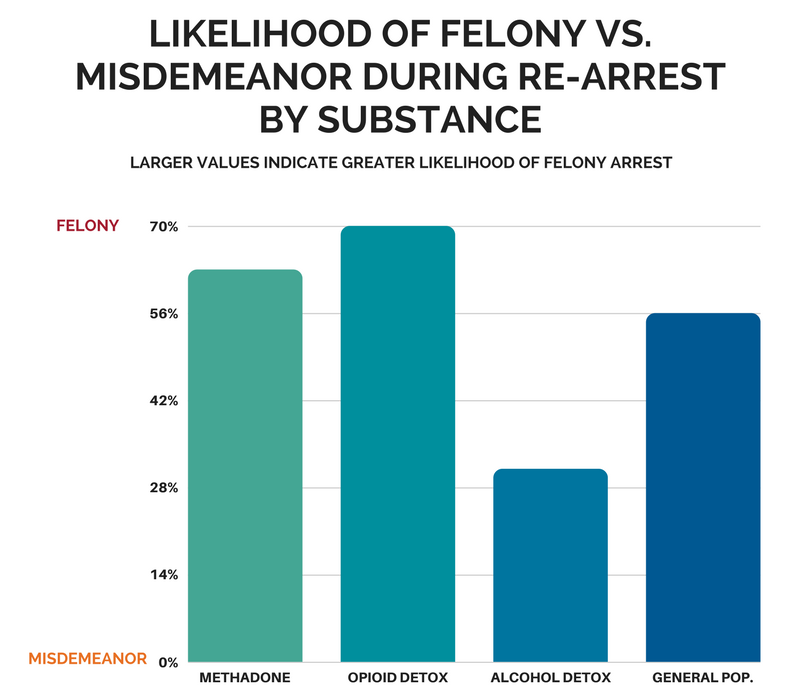
The main finding was that the likelihood of re-arrest in the year after release was higher in the opioid and alcohol detoxification than the general population and methadone patients, who were not different from each other. If re-arrested, though, methadone patients, along with opioid detoxification patients, were more likely to have been arrested for a felony rather than a misdemeanor (i.e., they were arrested for a presumably more serious offense).
Similarly, general population and methadone participants had longer time to re-arrest (286 and 276 days, respectively) compared to the opioid and alcohol detoxification participants (236 and 229 days, respectively). It is helpful to reiterate here that individuals who were not re-arrested during the year after release were automatically assigned a value of 366 days for re-arrest.
WHY IS THIS STUDY IMPORTANT
This study was an important contribution to research on criminal justice policies related to medications for opioid use disorder, even though authors did not examine recovery outcomes per se. A randomized trial could help determine whether there is a causal relationship between allowing inmates to remain on methadone or other medications for opioid use disorder versus mandating detoxification, and their criminal justice and substance use outcomes over time.
Preliminarily though, these findings suggest that remaining on methadone may be related to a lower likelihood of re-arrest, and a longer time to re-arrest, than if detoxified from methadone, a common practice in jails and prisons in the US.
It is important to mention that, when re-arrested, methadone participants were arrested for more serious crimes than individuals who were detoxified from opioids or alcohol. The design of the study, including an examination of existing criminal justice records, does not allow for a determination of why this was the case. It is possible that, because possession of a controlled substance apart from small amounts of marijuana is a felony in New Mexico where the study took place, that these arrests were related to illicit drug use. Overall, given the potentially greater societal impact of felonies relative to misdemeanors, this finding is worth investigating more in future studies.
- LIMITATIONS
-
- As authors note, the study did not randomize individuals already on methadone to either stay on methadone or to receive opioid detoxification. Nor did they control for factors that might be accounting for the different rates of re-arrest (e.g., days of incarceration for the index stay in jail). This was a program evaluation and authors made efforts to create good comparison groups for the methadone participants, by randomly selecting cases from individuals released during the same time period. This design was limited in its ability to determine, however, whether staying on methadone was responsible for the positive outcomes of this group.
- The study took place at one jail and with participants from one community with specific methadone programs. We do not know if these findings also apply to other settings.
NEXT STEPS
One next step could be to conduct a more controlled trial testing the benefits versus drawbacks of maintaining individuals on methadone who present to criminal justice settings. This study would ideally assess a range of outcomes, including both substance use, psychosocial functioning (e.g., employment and well-being), overdose, and likelihood of re-arrest.
BOTTOM LINE
- For individuals & families seeking recovery: For individuals receiving methadone who are arrested and required to spend time in jail, it may be best for them to remain on methadone rather than be detoxified, in terms of reducing someone’s likelihood of being arrested again. Not all criminal justice settings allow individuals to remain on methadone. More research is needed to investigate the benefits and drawbacks of remaining on methadone for individuals with opioid use disorder who are already receiving methadone in the community.
- For scientists: This naturalistic study suggested that for individuals receiving methadone who are arrested and required to spend time in jail, it may be best to remain on methadone rather than be detoxified, in terms of reducing rates of recidivism as well as time to re-arrest. While authors implemented features to increase their ability to make causal inferences, the study was limited both by the criminal justice and clinical records available to them, as well as the inability to use a randomized design in this program evaluation. The section, “What are the next steps in this line of research”, offers some ideas on potential future studies to help enhance the field’s knowledge in this area.
- For policy makers: For individuals receiving methadone who are arrested and required to spend time in jail, it may be best for them to remain on methadone rather than to be detoxified, in terms of reducing the likelihood of being arrested again. Not all criminal justice settings allow individuals to remain on methadone, however. While authors implemented features to increase their ability to make causal inferences, the study was limited both by the criminal justice and clinical records available to them, as well as the inability to use a randomized design in this program evaluation. More research is needed to investigate the benefits and drawbacks of policies that enable arrested individuals with opioid use disorder who are already receiving methadone in the community to remain on methadone.
- For treatment professionals and treatment systems: For individuals receiving methadone who are arrested and required to spend time in jail, it may be best to remain on methadone rather than be detoxified, in terms of reducing someone’s likelihood of being arrested again. Not all criminal justice settings allow individuals to remain on methadone, however. If they do, this study points to the potentially important role of communication and collaboration between the community-based methadone program and staff in the jail-based program. Overall, though, more research is needed to investigate the benefits and drawbacks of remaining on methadone for individuals with opioid use disorder who are already receiving methadone in the community.
CITATIONS
Westerberg, V. S., McCrady, B. S., Owens, M., & Guerin, P. (2016). Community-Based Methadone Maintenance in a Large Detention Center is Associated with Decreases in Inmate Recidivism. Journal of substance abuse treatment, 70, 1-6.
PHOTO CREDITS: Sarah Wurtz of The Inlander