
Can CBD reduce cocaine use and craving?
There are currently no FDA approved medications to treat cocaine use disorder. The administration of cannabidiol (CBD) – a non-psychoactive component of the cannabis plant – is associated with reduced craving and drug use for other substances, potentially by decreasing the brain’s reward response to substance use. In this study, the research team compared the effects of a high dose of CBD to placebo to determine whether this cannabinoid can reduce cocaine craving and use for individuals with cocaine use disorder.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
As of 2019, the World Drug Report indicates that over 20 million people use cocaine worldwide, and among those, at least 16% will be diagnosed with a cocaine use disorder. Cocaine use disorder is an individual and public health issue as it is associated with a number of life-impacting physical health effects (e.g., bronchitis, hepatitis C virus), mental health conditions, interpersonal problems, and premature death. One way to improve the lives of individuals who use cocaine, as well as to improve the disease burden of this disorder, is to find a treatment that reduces craving (or an intense desire) for cocaine because craving is an important predictor of cocaine relapse. While there are several psychosocial treatments shown to help people reduce cocaine use, there are currently no FDA approved medications for cocaine use disorder.
Human and animal research has shown that cannabidiol (CBD), a non-psychoactive component of the cannabis plant, may reduce drug use and other physical effects associated with cocaine and other stimulant use. In observational studies, people who use cocaine attribute their reduced cocaine use, craving, and negative physical effects (i.e., withdrawal symptoms) to their use of cannabis – suggesting a possible benefit of CBD for cocaine use disorder. There is also some evidence that CBD may be able to reduce cravings among individuals with heroin use disorder and cannabis use for those with cannabis use disorder. Among other potential effects on the brain, some animal research suggests CBD could help reduce the intensity of pleasurable experiences people have when using drugs like cocaine. CBD has few side effects in research trials and the side effects it does produce are relatively minor. In this study, researchers in Montreal, Quebec, Canada, investigated whether CBD helped reduce craving and cocaine use in adults with cocaine use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a double-blind, randomized, placebo-controlled trial that initially included 78 participants and was focused on comparing CBD to placebo on cue-induced cocaine craving during a 10-day inpatient detoxification stay as well as time to first cocaine use during a 12-week outpatient treatment phase. Participants ages 18 to 65 years with a diagnosis of cocaine use disorder who reported consuming cocaine in the past 2 weeks were eligible. Treatment randomization was stratified by sex and baseline severity of cocaine use disorder to ensure that the treatment and placebo groups were balanced on these variables. Ensuring group balance on key traits is important in smaller randomized trials like this one because even small non-equivalent differences on important variables that are not the variable of interest (i.e., CBD) can confuse the results. During the detoxification, participants received an oral solution of CBD or placebo, with 300 mg/day on day 1, 400 mg/day on days 2 and 3, and 800 mg/day for days 4 through 10. For the 12-week treatment, participants were provided weekly bottles of either CBD or placebo and instructed to take 800 mg each morning. Sixty-two participants – 35 in the CBD group and 27 in the placebo group – completed Phase 1, and 50 participants – 27 in the CBD group and 23 in the placebo group – completed both phases of the study. All participants had the option of attending a relapse prevention group session every week as well and received standard medical follow-up each month.
In addition to receiving CBD or placebo, this study involved a cue-induced craving experimental session during detoxification. On day 8 of the study, participants imagined three types of scenarios each for 5 minutes: (1) a neutral relaxing event (e.g., day at the beach), (2) a cocaine-use-related event (e.g., party with friends), and (3) a stressful situation (e.g., conflict with a friend). Scenario order during each session was randomized across participants to ensure that the effects of this cues were not due to the order in which scenarios were presented. After detoxification, participants continued to receive CBD vs. placebo for 12 weeks as an outpatient.
The primary outcomes were a) change in drug-cue-induced craving on a scale from 0 to 10 before and after the imagined scenario and b) time to first cocaine use during outpatient treatment determined by the number of days between detoxification discharge and the first day of cocaine use based on self-report and confirmed by toxicology screen. Secondary outcomes included stress-induced craving during the cue exposures and cocaine use based on the percentage of positive urine toxicology screens conducted at each weekly follow-up. Exploratory outcomes were daily cocaine craving (assessed every 2 days during detoxification and every 2 weeks during treatment), cocaine withdrawal symptoms (examined every 2 days during detoxification and monthly during treatment), and “sustained abstinence” defined as 21 consecutive days without any cocaine use.
The initial sample of 78 participants were 46 years old on average; 86% identified as White (researchers did not specify race/ethnicity of the other 14%); and 18% identified as female. Clinically, 95% were diagnosed with severe cocaine use disorder – meaning they had 6 or more out of 11 DSM-5 symptoms – and 55% preferred to consume cocaine by smoking while 31% preferred intranasal use. Small sub-groups, from 5 to 10%, had another substance use disorder, including alcohol, cannabis, or other stimulants. Of note, individuals with other substance use disorders that were severe (6+ symptoms) were excluded, likely accounting for smaller sub-groups of individuals with co-occurring substance use disorder.
WHAT DID THIS STUDY FIND?
CBD did not improve cocaine craving or withdrawal.
Participants receiving CBD (vs. placebo) experienced similar increases in their subjective cravings for cocaine following the cocaine-related cue and the stress cue. Self-reported cocaine craving and withdrawal symptoms across the study were also similar across groups.
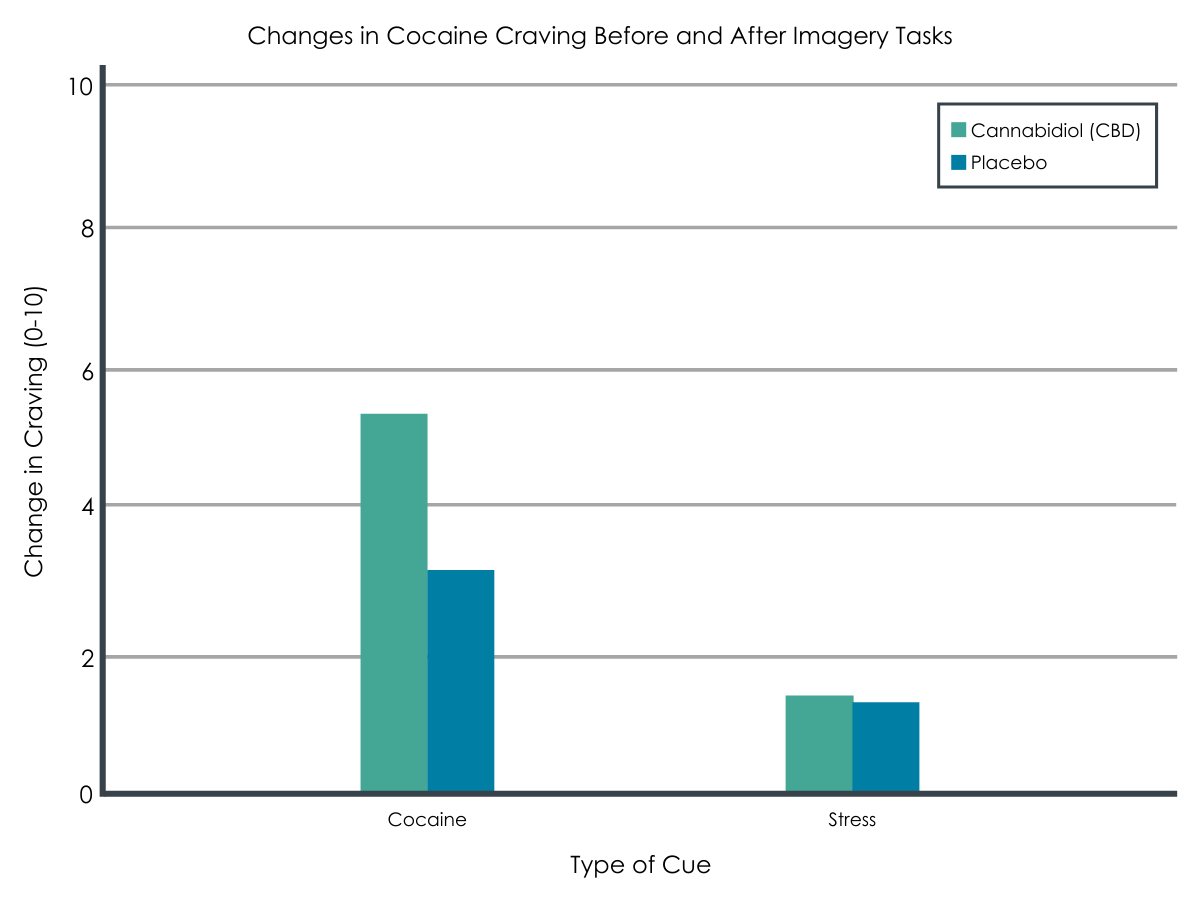
Adapted from Mongeau-Pérusse et al., 2021. In response to imagery including both cocaine cues (left) and stress cues (right), participants receiving CBD and placebo had similar craving increases from before to after the task.
CBD did not reduce cocaine use or improve time to first cocaine use.
Time to first cocaine use was similar for participants receiving CBD or placebo. The median number of days between discharge following detoxification and cocaine use was 4 days for the CBD group and 7 days for the placebo group. The proportion of participants reaching sustained abstinence – 21 consecutive days – was also similar for both groups, with 21% in the CBD group and 41% in placebo. There also was a similar proportion of participants who used cocaine (as determined by positive urine tests) during Phase 2. Likewise, the number of self-reported cocaine use days across the study was similar across groups with 32 days of cocaine use in the CBD group and 29 in the placebo group.
Few receiving CBD experienced side effects.
CBD at 800 mg/day was generally well tolerated in this study. Among those who received CBD, about 43% reported at least 1 unwanted side effect of the medication. The most frequently reported side effects were diarrhea and nausea.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study was a well-conducted rigorous randomized placebo-controlled trial that tested whether CBD could reduce cocaine craving and time to first use after a period of medically-supervised abstinence during inpatient detoxification. CBD was also well tolerated in this sample. CBD did no better than placebo in this sample of adults with (primarily severe) cocaine use disorder. Researchers and clinicians have been enthusiastic about the potential for CBD as an addiction treatment. Findings from this study, however, do not support the use of CBD in treating cocaine use disorder specifically.
It is possible that the clinical severity of this sample may have affected study findings (94% severe cocaine use disorder), as an animal study showed that CBD reduced cocaine self-administration in low doses but not high doses of cocaine. That said, considering findings from another study that found no differences between CBD and placebo in improving cocaine use outcomes, the most likely explanation of study findings to date is that CBD is not an efficacious intervention for cocaine use disorder. The ultimate sample size (78 in Phase 1 and 62 in Phase 2) did not reach their target sample of 110, which was chosen to given them the best chance of detecting a difference between the CBD and placebo groups if one existing (referred to as statistical power). Though it is unclear what procedural barriers specifically accounted for this under-recruitment, given that placebo descriptively outperformed CBD (e.g., 29 vs. 32 % days of cocaine use, respectively), even a larger sample would not have resulted in observed benefit for CBD.
Worth noting, however, is that CBD outperformed placebo in reducing heroin craving and stress following a drug cue in a sample of people with heroin use disorder. CBD also reduced cannabis use and tobacco use relative to placebo across 24 weeks among individuals with cannabis use disorder. This effect of CBD on tobacco use has been replicated. Despite clear efforts to do so, no effective pharmacological treatments have been developed for cocaine use disorder to date. Advancing research on novel pharmacological treatments as well as psychosocial treatments, and studies of how they might be optimally combined, for cocaine use disorder is critically needed to address the harms associated with this disorder.
- LIMITATIONS
-
- The sample included predominantly White males, which limits the generalizability of findings to other demographic groups.
- Almost all participants were diagnosed with a severe cocaine use disorder (94% of the sample), so this study cannot test the efficacy of CBD on craving and cocaine use among those with milder forms of cocaine use disorder.
- Most participants reported that they primarily used cocaine via smoking rather than intranasally. Also, small sub-groups met criteria for another substance use disorder, unlike the majority of trials where co-occurring substance use disorders are the norm. Of note, as well, this study took place in Montreal, Quebec, Canada. Whether these findings can be applied to other samples of individuals with cocaine use disorder, where intranasal use and co-occurring substance use disorders may be more common, and to other settings in Canada (e.g., Toronto, Ontario) and the US is uncertain.
- The ultimate sample size was 61, including 34 in the CBD group and 27 in the placebo group, lower than the target sample size of 110 (55 per group) chosen so the study would be powered to detect a statistically significant effect if it existed in the data. The final sample size significantly reduced statistical power, which increased the likelihood of not detecting a significant effect when it actually existed in the data (i.e., Type II error). Therefore, it is also worth noting that placebo descriptively outperformed CBD (e.g., the largest difference on sustained abstinence, 41% placebo vs. 21% CBD, a p-value of .09). A larger sample may have resulted in statistical significance and also given a more accurate estimate of potential differences between CBD and placebo.
- The study did not include information about the nature of relapse prevention groups participants could attend, nor the degree to which participants attended these groups. As such, the relationship between group therapy attendance and outcomes, and whether this relationship differed by CBD vs. placebo, is unknown.
BOTTOM LINE
In a sample of individuals with mostly severe cocaine use disorder, researchers tested whether cannabidiol (CBD) reduced cocaine craving during inpatient detoxification and time to first use during 12-week outpatient treatment. Overall, despite being well tolerated, CBD did not improve cocaine use outcomes, which is consistent with a similar prior study. Taken together, it is possible CBD improves outcomes for other substances (e.g., opioids, tobacco, cannabis), but this is not the case for cocaine use disorder. Developing and implementing efficacious pharmacological treatments for cocaine use disorder, while continuing to amplify and build on existing empirically-supported psychosocial approaches, remains a high priority.
- For individuals and families seeking recovery: Individuals with cocaine use disorder or those who use cocaine and would like to reduce their use should be aware that CBD does not improve cocaine craving and risk for recurrence of use. Until an effective pharmacological treatment is developed, psychosocial treatments that have been shown to help with cocaine use disorder, such as contingency management, 12-step facilitation, and cognitive-behavioral therapy are recommended for individuals hoping to resolve their cocaine use disorder.
- For treatment professionals and treatment systems: CBD was not supported as an effective treatment for cocaine craving and risk for recurrence of use. Because no other effective pharmacological treatments for cocaine use disorder have been identified, psychosocial interventions with more consistent evidence of improved cocaine treatment outcomes are recommended instead (e.g., contingency management, 12-step facilitation, and cognitive-behavioral therapy).
- For scientists: In this study, the research team used a rigorous randomized placebo-controlled trial to test the effectiveness of CBD (vs. placebo) on cocaine craving and time to first cocaine use. This study extended a prior study that found null results when administering a lower dose of CBD (300 mg vs. 800 mg in the present study). Despite the increased dose, however, the effects of CBD remained null, suggesting that it may not be helpful for the treatment of cocaine use disorder. Future research may benefit from identifying and developing novel pharmacological treatments for cocaine use disorder. This could then complement existing psychosocial treatments for cocaine use disorder (e.g., contingency management, 12-step facilitation, and cognitive-behavioral therapy) which have been shown to be beneficial.
- For policy makers: Despite well-designed studies, future research investigating whether CBD is effective for treating cocaine use disorder may not be beneficial. Instead, more funding is needed to develop novel and effective pharmacological treatments for cocaine use disorder, as this has not been established to date. Doing so may bolster an existing effective psychosocial treatment for cocaine use disorder – contingency management – which has been shown to act synergistically with pharmacotherapy.
CITATIONS
Mongeau-Pérusse, V., Brissette, S., Bruneau, J., Conrod, P., Dubreucq, S., Gazil, G., Stip, E., & Jutras-Aswad, D. (2021). Cannabidiol as a treatment for craving and relapse in individuals with cocaine use disorder: a randomized placebo-controlled trial. Addiction, 116(9), 2431-2442. doi: 10.1111/add.15417