Indicators of “success” in buprenorphine treatment for opioid use disorder
Opioid abstinence and treatment retention are common markers of success for individuals receiving opioid use disorder medications. Going beyond these markers to include all desired outcomes for buprenorphine treatment in both patients and prescribers may increase how readily buprenorphine services are adopted in clinical practice. This study asked physicians prescribing these medications in primary care as well as their patients receiving the medications what they believe are indicators of treatment success.
Methadone and buprenorphine are FDA-approved medications used to treat individuals with opioid use disorder. Although they have been prescribed since the 1960’s, there is little consensus on definitions of successful outcomes for those receiving these medications.Both medicationshave been found to reduce overdose mortality and use of opioids. Yet, opioid use disorder impacts multiple domains of an individual’s life, and treatment goals for many patients extend beyond survival and opioid use. Understanding what success means to patients receiving medications for opioid use disorder and clinicians prescribing the medicationis an important yet difficult undertaking. Examining what success means to these key groups may improve service delivery, patient experience, and ultimately the lives of individuals with opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
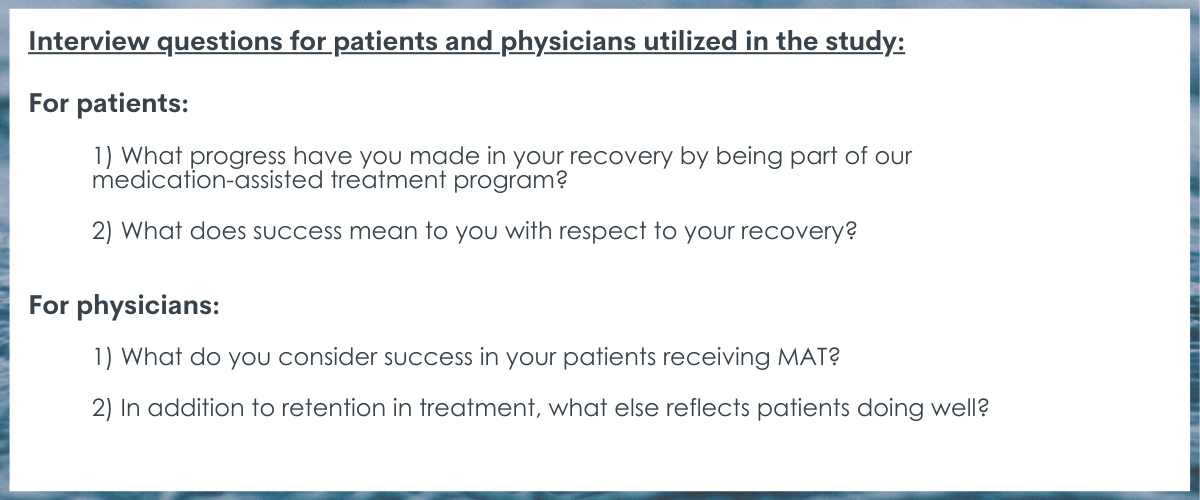
This was a qualitative study that used individual interviews with patients and physicians to explore what they perceive as indicators of success in treatment for opioid use disorder prescribed medications. A total of 14 physicians and 18 patients were interviewed representing 2 university-affiliated family medicine clinics in Minneapolis, Minnesota. All interviews were conducted between October 2020 and February 2021.
Participants were primary care physicians and patients with opioid use disorder being treated with buprenorphine. Physicians were faculty and residents in family medicine that also had DATA 2000 waivers, which was previously required to prescribe buprenorphine. All residents were in their 3rd post-graduate-year (PGY 3), had received previous training, and prescribed medication for opioid use disorder to at least 25 patients in the prior year. Patients had an opioid use disorder diagnosis and had received a buprenorphine prescription between April 1, 2020, and June 30, 2020. Eligible patients were identified using a retrospective analysis of electronic health records and recommended by physicians, which included one of the study authors who sees patients at the clinic.
After recruitment, interviews were conducted with the physicians and patients via telephone. Each interview lasted 20-30 minutes and featured key questions about indicators of success.
Fourteen physicians and 18 patients completed interviews. The physicians consisted of 7 faculty and 7 residents who had been waivered to prescribe buprenorphine for an average of 5.7 years. Physicians reported an average age of 34.6, and they all identified as white, non-Hispanic with 8 identifying as female. Ten of the physicians held doctorates in medicine (MD) while 4 held Doctor of Osteopathic Medicine degrees.
The patients were long-term recipients of medication for opioid use disorder and reported an average of 2.5 years of participation in the clinic’s program. They were, on average, 38.1 years old. Eight were female and 14 identified as white, non-Hispanic.
WHAT DID THIS STUDY FIND?
Indicators of medication for opioid use disorder treatment success go beyond abstinence.
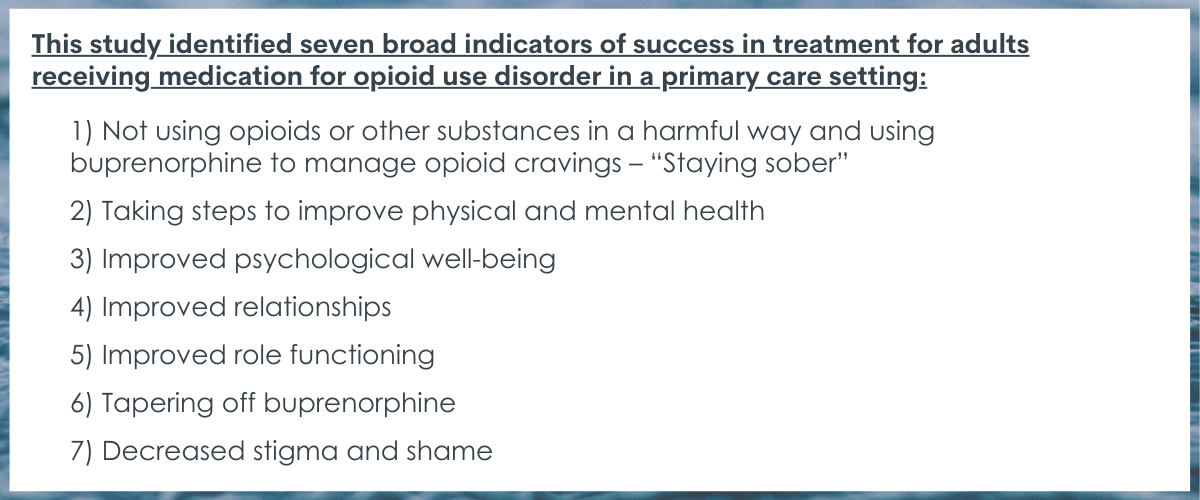
Patients and physicians reported abstinence from opioids and other substances as part of successful treatment. However, both groups described a concept of treatment success that went beyond treatment to include health and well-being more generally. Action steps were listed that identified working towards improving physical and mental health (e.g., quitting smoking, self-care). Additionally, the outcomes of action steps were also described as improvements in psychological well-being such as feeling happier or feeling “normal.” Relationships and roles were two other groupings of indicators for success. Improved relationships were discussed as both interconnectedness between patients and other peers as well as between patients and physicians. Patients and physicians also identified success as the improvement in important life roles and functions such as getting a job, going back to school, getting a driver’s license, and setting/meeting life goals.
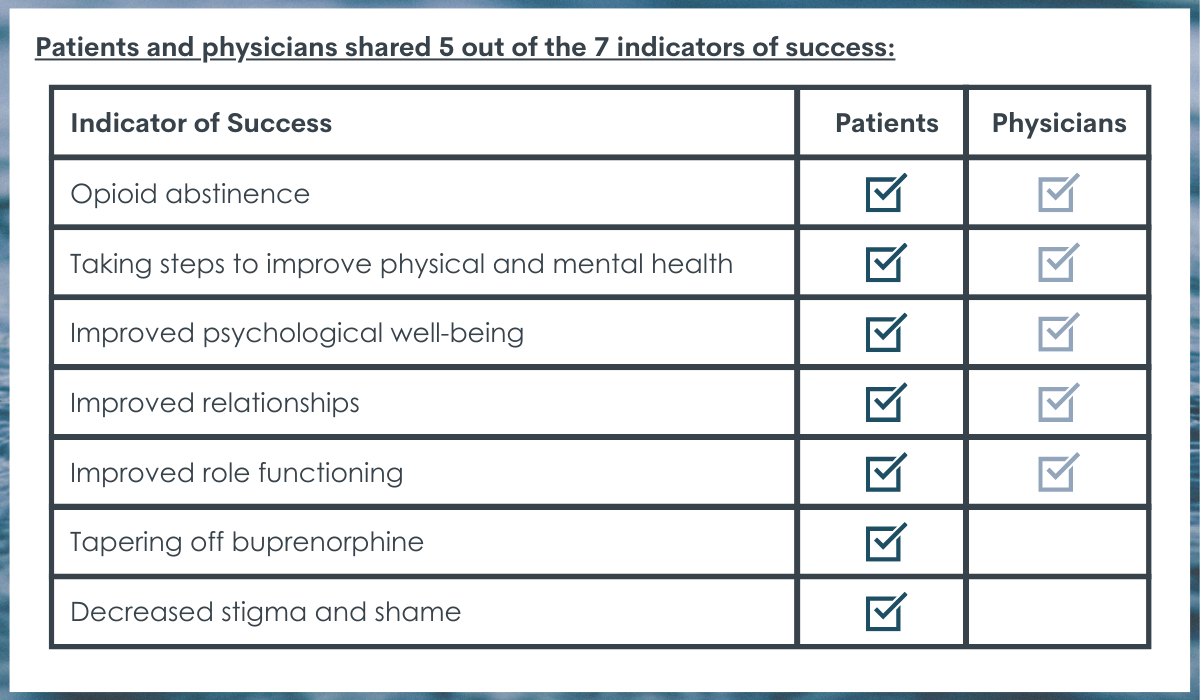
Patients and physicians shared five of the seven indicators.
Patients and physicians shared similar indicators of success, but patients also uniquely identified tapering off buprenorphine and decreased self-stigma and shame as two important measures of success. Tapering off medication was strongly endorsed by patients, even though patients had been using the medication for 2.5 years, on average, through the clinic. However, only one physician noted tapering as a possible goal or measure of success. Similarly, patients described a shift from feeling their identity was consumed by substances to reduced internalized stigma and shame, which was marked by patient’s ability to be more open and accepting of having an opioid use disorder and its associated challenges.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Definitions of treatment success can significantly influence patient goals and programs. Traditionally, clinicians and researchers have defined opioid use disorder treatment success as abstinence and treatment retention. The findings from this study showed that patients receiving buprenorphine and their primary care prescribers identified several makers of success beyond opioid or other substance use. Wellness and functioning improvements were echoed by both groups. The identification of goals other than reduction of opioid use pinpoint a potential need for clinicians to provide additional supports and/or linkage to other resources for patients to pursue improvements in these other areas. Of note, however, is the potential need for structural and community supports to fill existing gaps. Additionally, it is possible that one’s ability to make progress in some domains is dependent on first making progress in other domains. For example, addressing harmful substance use (i.e., via abstinence or harm reduction), medication adherence, and others may be needed first to provide the foundation for subsequent improvements in quality of life and better functioning.
Treatment retention has traditionally been an indicator of treatment success. However, primary care-based medication for opioid use disorder does not have a predefined length of treatment. While studies may show improvements in mortality after a year of medication use and reductions in overdose risk after 6 months, there is not a standard length of care for medication treatment. This lack of standardization can create a tension between providers and their patients. Providers may recognize the increased chances of relapse and consequences following the discontinuation of medication, yet adults receiving medication may see tapering off and eventual discontinuation as a desirable treatment goal. This study identified these different perceptions of medication treatment success in that tapering was a goal identified by most patients, yet only one physician mentioned tapering may be a goal for patients. Providers, researchers, and adults in treatment may all benefit from the inclusion of a mix of patient-centered and evidence-based treatment goals. Furthermore, this study implies that more work is needed to understand how and when to help adults safely taper medications for opioid use disorder.
As optimal recovery and treatment outcomes continue to be explored and identified, it will be important to consider the views of individuals pursuing recovery and/or treatment. A recent report by Community Catalyst, Faces and Voices of Recovery, and the American Society of Addiction Medicine found extensive diversity in priorities among more than 800 individuals with lived experience, with no one priority shared among most participants. Even so, and more specifically, little is known about definitions of success among adults prescribed medication for opioid use disorder and the physicians who prescribe the medications. Although medications have been shown to be helpful in treatment, the course of treatment and the potential discontinuation of medications may be contested among patients and physicians. This study highlighted makers of medication for opioid use disorder treatment outcomes from a patient-centered perspective, which was found to differ to some degree from a physician-centered perspective.
The physicians and researchers identified patients receiving medications for opioid use disorder for participation but did not specify how these decisions were made. Thus, the sample may be biased in some or other fashion, and the patients selected for participation may not represent the clinic populations they come from or opioid use disorder patients taking buprenorphine more generally.
All patients had received medications for opioid use disorder at the two clinics for an average of 2.5 years, which implies they were a relatively stable and adhered to the clinic’s guidelines and direction. The stability presented in the sample may skew the perceptions of success compared to those with less time receiving medications for opioid use disorder. For example, patients newly prescribed medications for opioid use disorder may be focused on stabilizing and surviving with little thought towards long-term goals such as tapering off medication. Patients with more stability, however, may be more likely to consider other goals such as tapering.
The study, like all qualitative studies, is subject to the lines of inquiry explored by the research team. The questions the researchers asked during the interviews might impact the themes expressed by patients and physicians as well as their implications.
BOTTOM LINE
This qualitative study found that patients receiving medication for opioid use disorder and their prescribing physicians have goals that include, but goes beyond, reductions in substance use. Indicators of success include taking action to improve health and well-being, improvements in health and well-being, improvements in relationships, advances in role functioning (e.g., getting a job), and being abstinent from substances. Additionally, patients identified tapering of medication and reduced stigma and shame as indicators of success. These findings suggest that goals beyond reduced opioid use and treatment retention may be of interest to patients and their doctors and some of these desirable goals may be different for patients and their prescribers.
For individuals and families seeking recovery: This study highlights how individuals receiving medications for opioid use disorder may have goals to improve health and happiness that extend beyond opioid use. Given that you too may have these recovery goals, you may wish to speak to your treatment and recovery support providers about how best to approach these recovery goals beyond reductions in or elimination of substance use.
For treatment professionals and treatment systems: This study found that patients receiving buprenorphine and their prescribing physicians perceive success to include abstinence but to also include indicators of success such as improvements in health and well-being, improvements in relationship, and advances in role functioning (e.g., getting a job). Exploring and supporting patient goals beside reduced substance use may improve patient experiences and outcomes.
For scientists:This qualitative study recruited patients receiving buprenorphine and their prescribing physicians from two primary care-based clinics in Minnesota. Although findings here echo previous studies supporting conceptualizations of treatment success and recovery that extend beyond abstinence, future research should explore perceptions of success among a more diverse sample. Geographic, racial/ethnic, cultural, and history of treatment may all influence perceptions of success. Future studies may also explore how to effectively incorporate perceptions of success and their associated goals into treatment planning. Furthermore, identifying structural and community resources that support these goals will likely improve patient outcomes.
For policy makers: Funding and policy that helps patients accomplish their goals beyond substance use may help to improve patient engagement, treatment satisfaction, and ultimately, enhance the chances of ongoing opioid use disorder remission.
Methadone and buprenorphine are FDA-approved medications used to treat individuals with opioid use disorder. Although they have been prescribed since the 1960’s, there is little consensus on definitions of successful outcomes for those receiving these medications.Both medicationshave been found to reduce overdose mortality and use of opioids. Yet, opioid use disorder impacts multiple domains of an individual’s life, and treatment goals for many patients extend beyond survival and opioid use. Understanding what success means to patients receiving medications for opioid use disorder and clinicians prescribing the medicationis an important yet difficult undertaking. Examining what success means to these key groups may improve service delivery, patient experience, and ultimately the lives of individuals with opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
This was a qualitative study that used individual interviews with patients and physicians to explore what they perceive as indicators of success in treatment for opioid use disorder prescribed medications. A total of 14 physicians and 18 patients were interviewed representing 2 university-affiliated family medicine clinics in Minneapolis, Minnesota. All interviews were conducted between October 2020 and February 2021.
Participants were primary care physicians and patients with opioid use disorder being treated with buprenorphine. Physicians were faculty and residents in family medicine that also had DATA 2000 waivers, which was previously required to prescribe buprenorphine. All residents were in their 3rd post-graduate-year (PGY 3), had received previous training, and prescribed medication for opioid use disorder to at least 25 patients in the prior year. Patients had an opioid use disorder diagnosis and had received a buprenorphine prescription between April 1, 2020, and June 30, 2020. Eligible patients were identified using a retrospective analysis of electronic health records and recommended by physicians, which included one of the study authors who sees patients at the clinic.
After recruitment, interviews were conducted with the physicians and patients via telephone. Each interview lasted 20-30 minutes and featured key questions about indicators of success.
Fourteen physicians and 18 patients completed interviews. The physicians consisted of 7 faculty and 7 residents who had been waivered to prescribe buprenorphine for an average of 5.7 years. Physicians reported an average age of 34.6, and they all identified as white, non-Hispanic with 8 identifying as female. Ten of the physicians held doctorates in medicine (MD) while 4 held Doctor of Osteopathic Medicine degrees.
The patients were long-term recipients of medication for opioid use disorder and reported an average of 2.5 years of participation in the clinic’s program. They were, on average, 38.1 years old. Eight were female and 14 identified as white, non-Hispanic.
WHAT DID THIS STUDY FIND?
Indicators of medication for opioid use disorder treatment success go beyond abstinence.
Patients and physicians reported abstinence from opioids and other substances as part of successful treatment. However, both groups described a concept of treatment success that went beyond treatment to include health and well-being more generally. Action steps were listed that identified working towards improving physical and mental health (e.g., quitting smoking, self-care). Additionally, the outcomes of action steps were also described as improvements in psychological well-being such as feeling happier or feeling “normal.” Relationships and roles were two other groupings of indicators for success. Improved relationships were discussed as both interconnectedness between patients and other peers as well as between patients and physicians. Patients and physicians also identified success as the improvement in important life roles and functions such as getting a job, going back to school, getting a driver’s license, and setting/meeting life goals.
Patients and physicians shared five of the seven indicators.
Patients and physicians shared similar indicators of success, but patients also uniquely identified tapering off buprenorphine and decreased self-stigma and shame as two important measures of success. Tapering off medication was strongly endorsed by patients, even though patients had been using the medication for 2.5 years, on average, through the clinic. However, only one physician noted tapering as a possible goal or measure of success. Similarly, patients described a shift from feeling their identity was consumed by substances to reduced internalized stigma and shame, which was marked by patient’s ability to be more open and accepting of having an opioid use disorder and its associated challenges.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Definitions of treatment success can significantly influence patient goals and programs. Traditionally, clinicians and researchers have defined opioid use disorder treatment success as abstinence and treatment retention. The findings from this study showed that patients receiving buprenorphine and their primary care prescribers identified several makers of success beyond opioid or other substance use. Wellness and functioning improvements were echoed by both groups. The identification of goals other than reduction of opioid use pinpoint a potential need for clinicians to provide additional supports and/or linkage to other resources for patients to pursue improvements in these other areas. Of note, however, is the potential need for structural and community supports to fill existing gaps. Additionally, it is possible that one’s ability to make progress in some domains is dependent on first making progress in other domains. For example, addressing harmful substance use (i.e., via abstinence or harm reduction), medication adherence, and others may be needed first to provide the foundation for subsequent improvements in quality of life and better functioning.
Treatment retention has traditionally been an indicator of treatment success. However, primary care-based medication for opioid use disorder does not have a predefined length of treatment. While studies may show improvements in mortality after a year of medication use and reductions in overdose risk after 6 months, there is not a standard length of care for medication treatment. This lack of standardization can create a tension between providers and their patients. Providers may recognize the increased chances of relapse and consequences following the discontinuation of medication, yet adults receiving medication may see tapering off and eventual discontinuation as a desirable treatment goal. This study identified these different perceptions of medication treatment success in that tapering was a goal identified by most patients, yet only one physician mentioned tapering may be a goal for patients. Providers, researchers, and adults in treatment may all benefit from the inclusion of a mix of patient-centered and evidence-based treatment goals. Furthermore, this study implies that more work is needed to understand how and when to help adults safely taper medications for opioid use disorder.
As optimal recovery and treatment outcomes continue to be explored and identified, it will be important to consider the views of individuals pursuing recovery and/or treatment. A recent report by Community Catalyst, Faces and Voices of Recovery, and the American Society of Addiction Medicine found extensive diversity in priorities among more than 800 individuals with lived experience, with no one priority shared among most participants. Even so, and more specifically, little is known about definitions of success among adults prescribed medication for opioid use disorder and the physicians who prescribe the medications. Although medications have been shown to be helpful in treatment, the course of treatment and the potential discontinuation of medications may be contested among patients and physicians. This study highlighted makers of medication for opioid use disorder treatment outcomes from a patient-centered perspective, which was found to differ to some degree from a physician-centered perspective.
The physicians and researchers identified patients receiving medications for opioid use disorder for participation but did not specify how these decisions were made. Thus, the sample may be biased in some or other fashion, and the patients selected for participation may not represent the clinic populations they come from or opioid use disorder patients taking buprenorphine more generally.
All patients had received medications for opioid use disorder at the two clinics for an average of 2.5 years, which implies they were a relatively stable and adhered to the clinic’s guidelines and direction. The stability presented in the sample may skew the perceptions of success compared to those with less time receiving medications for opioid use disorder. For example, patients newly prescribed medications for opioid use disorder may be focused on stabilizing and surviving with little thought towards long-term goals such as tapering off medication. Patients with more stability, however, may be more likely to consider other goals such as tapering.
The study, like all qualitative studies, is subject to the lines of inquiry explored by the research team. The questions the researchers asked during the interviews might impact the themes expressed by patients and physicians as well as their implications.
BOTTOM LINE
This qualitative study found that patients receiving medication for opioid use disorder and their prescribing physicians have goals that include, but goes beyond, reductions in substance use. Indicators of success include taking action to improve health and well-being, improvements in health and well-being, improvements in relationships, advances in role functioning (e.g., getting a job), and being abstinent from substances. Additionally, patients identified tapering of medication and reduced stigma and shame as indicators of success. These findings suggest that goals beyond reduced opioid use and treatment retention may be of interest to patients and their doctors and some of these desirable goals may be different for patients and their prescribers.
For individuals and families seeking recovery: This study highlights how individuals receiving medications for opioid use disorder may have goals to improve health and happiness that extend beyond opioid use. Given that you too may have these recovery goals, you may wish to speak to your treatment and recovery support providers about how best to approach these recovery goals beyond reductions in or elimination of substance use.
For treatment professionals and treatment systems: This study found that patients receiving buprenorphine and their prescribing physicians perceive success to include abstinence but to also include indicators of success such as improvements in health and well-being, improvements in relationship, and advances in role functioning (e.g., getting a job). Exploring and supporting patient goals beside reduced substance use may improve patient experiences and outcomes.
For scientists:This qualitative study recruited patients receiving buprenorphine and their prescribing physicians from two primary care-based clinics in Minnesota. Although findings here echo previous studies supporting conceptualizations of treatment success and recovery that extend beyond abstinence, future research should explore perceptions of success among a more diverse sample. Geographic, racial/ethnic, cultural, and history of treatment may all influence perceptions of success. Future studies may also explore how to effectively incorporate perceptions of success and their associated goals into treatment planning. Furthermore, identifying structural and community resources that support these goals will likely improve patient outcomes.
For policy makers: Funding and policy that helps patients accomplish their goals beyond substance use may help to improve patient engagement, treatment satisfaction, and ultimately, enhance the chances of ongoing opioid use disorder remission.
Methadone and buprenorphine are FDA-approved medications used to treat individuals with opioid use disorder. Although they have been prescribed since the 1960’s, there is little consensus on definitions of successful outcomes for those receiving these medications.Both medicationshave been found to reduce overdose mortality and use of opioids. Yet, opioid use disorder impacts multiple domains of an individual’s life, and treatment goals for many patients extend beyond survival and opioid use. Understanding what success means to patients receiving medications for opioid use disorder and clinicians prescribing the medicationis an important yet difficult undertaking. Examining what success means to these key groups may improve service delivery, patient experience, and ultimately the lives of individuals with opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
This was a qualitative study that used individual interviews with patients and physicians to explore what they perceive as indicators of success in treatment for opioid use disorder prescribed medications. A total of 14 physicians and 18 patients were interviewed representing 2 university-affiliated family medicine clinics in Minneapolis, Minnesota. All interviews were conducted between October 2020 and February 2021.
Participants were primary care physicians and patients with opioid use disorder being treated with buprenorphine. Physicians were faculty and residents in family medicine that also had DATA 2000 waivers, which was previously required to prescribe buprenorphine. All residents were in their 3rd post-graduate-year (PGY 3), had received previous training, and prescribed medication for opioid use disorder to at least 25 patients in the prior year. Patients had an opioid use disorder diagnosis and had received a buprenorphine prescription between April 1, 2020, and June 30, 2020. Eligible patients were identified using a retrospective analysis of electronic health records and recommended by physicians, which included one of the study authors who sees patients at the clinic.
After recruitment, interviews were conducted with the physicians and patients via telephone. Each interview lasted 20-30 minutes and featured key questions about indicators of success.
Fourteen physicians and 18 patients completed interviews. The physicians consisted of 7 faculty and 7 residents who had been waivered to prescribe buprenorphine for an average of 5.7 years. Physicians reported an average age of 34.6, and they all identified as white, non-Hispanic with 8 identifying as female. Ten of the physicians held doctorates in medicine (MD) while 4 held Doctor of Osteopathic Medicine degrees.
The patients were long-term recipients of medication for opioid use disorder and reported an average of 2.5 years of participation in the clinic’s program. They were, on average, 38.1 years old. Eight were female and 14 identified as white, non-Hispanic.
WHAT DID THIS STUDY FIND?
Indicators of medication for opioid use disorder treatment success go beyond abstinence.
Patients and physicians reported abstinence from opioids and other substances as part of successful treatment. However, both groups described a concept of treatment success that went beyond treatment to include health and well-being more generally. Action steps were listed that identified working towards improving physical and mental health (e.g., quitting smoking, self-care). Additionally, the outcomes of action steps were also described as improvements in psychological well-being such as feeling happier or feeling “normal.” Relationships and roles were two other groupings of indicators for success. Improved relationships were discussed as both interconnectedness between patients and other peers as well as between patients and physicians. Patients and physicians also identified success as the improvement in important life roles and functions such as getting a job, going back to school, getting a driver’s license, and setting/meeting life goals.
Patients and physicians shared five of the seven indicators.
Patients and physicians shared similar indicators of success, but patients also uniquely identified tapering off buprenorphine and decreased self-stigma and shame as two important measures of success. Tapering off medication was strongly endorsed by patients, even though patients had been using the medication for 2.5 years, on average, through the clinic. However, only one physician noted tapering as a possible goal or measure of success. Similarly, patients described a shift from feeling their identity was consumed by substances to reduced internalized stigma and shame, which was marked by patient’s ability to be more open and accepting of having an opioid use disorder and its associated challenges.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Definitions of treatment success can significantly influence patient goals and programs. Traditionally, clinicians and researchers have defined opioid use disorder treatment success as abstinence and treatment retention. The findings from this study showed that patients receiving buprenorphine and their primary care prescribers identified several makers of success beyond opioid or other substance use. Wellness and functioning improvements were echoed by both groups. The identification of goals other than reduction of opioid use pinpoint a potential need for clinicians to provide additional supports and/or linkage to other resources for patients to pursue improvements in these other areas. Of note, however, is the potential need for structural and community supports to fill existing gaps. Additionally, it is possible that one’s ability to make progress in some domains is dependent on first making progress in other domains. For example, addressing harmful substance use (i.e., via abstinence or harm reduction), medication adherence, and others may be needed first to provide the foundation for subsequent improvements in quality of life and better functioning.
Treatment retention has traditionally been an indicator of treatment success. However, primary care-based medication for opioid use disorder does not have a predefined length of treatment. While studies may show improvements in mortality after a year of medication use and reductions in overdose risk after 6 months, there is not a standard length of care for medication treatment. This lack of standardization can create a tension between providers and their patients. Providers may recognize the increased chances of relapse and consequences following the discontinuation of medication, yet adults receiving medication may see tapering off and eventual discontinuation as a desirable treatment goal. This study identified these different perceptions of medication treatment success in that tapering was a goal identified by most patients, yet only one physician mentioned tapering may be a goal for patients. Providers, researchers, and adults in treatment may all benefit from the inclusion of a mix of patient-centered and evidence-based treatment goals. Furthermore, this study implies that more work is needed to understand how and when to help adults safely taper medications for opioid use disorder.
As optimal recovery and treatment outcomes continue to be explored and identified, it will be important to consider the views of individuals pursuing recovery and/or treatment. A recent report by Community Catalyst, Faces and Voices of Recovery, and the American Society of Addiction Medicine found extensive diversity in priorities among more than 800 individuals with lived experience, with no one priority shared among most participants. Even so, and more specifically, little is known about definitions of success among adults prescribed medication for opioid use disorder and the physicians who prescribe the medications. Although medications have been shown to be helpful in treatment, the course of treatment and the potential discontinuation of medications may be contested among patients and physicians. This study highlighted makers of medication for opioid use disorder treatment outcomes from a patient-centered perspective, which was found to differ to some degree from a physician-centered perspective.
The physicians and researchers identified patients receiving medications for opioid use disorder for participation but did not specify how these decisions were made. Thus, the sample may be biased in some or other fashion, and the patients selected for participation may not represent the clinic populations they come from or opioid use disorder patients taking buprenorphine more generally.
All patients had received medications for opioid use disorder at the two clinics for an average of 2.5 years, which implies they were a relatively stable and adhered to the clinic’s guidelines and direction. The stability presented in the sample may skew the perceptions of success compared to those with less time receiving medications for opioid use disorder. For example, patients newly prescribed medications for opioid use disorder may be focused on stabilizing and surviving with little thought towards long-term goals such as tapering off medication. Patients with more stability, however, may be more likely to consider other goals such as tapering.
The study, like all qualitative studies, is subject to the lines of inquiry explored by the research team. The questions the researchers asked during the interviews might impact the themes expressed by patients and physicians as well as their implications.
BOTTOM LINE
This qualitative study found that patients receiving medication for opioid use disorder and their prescribing physicians have goals that include, but goes beyond, reductions in substance use. Indicators of success include taking action to improve health and well-being, improvements in health and well-being, improvements in relationships, advances in role functioning (e.g., getting a job), and being abstinent from substances. Additionally, patients identified tapering of medication and reduced stigma and shame as indicators of success. These findings suggest that goals beyond reduced opioid use and treatment retention may be of interest to patients and their doctors and some of these desirable goals may be different for patients and their prescribers.
For individuals and families seeking recovery: This study highlights how individuals receiving medications for opioid use disorder may have goals to improve health and happiness that extend beyond opioid use. Given that you too may have these recovery goals, you may wish to speak to your treatment and recovery support providers about how best to approach these recovery goals beyond reductions in or elimination of substance use.
For treatment professionals and treatment systems: This study found that patients receiving buprenorphine and their prescribing physicians perceive success to include abstinence but to also include indicators of success such as improvements in health and well-being, improvements in relationship, and advances in role functioning (e.g., getting a job). Exploring and supporting patient goals beside reduced substance use may improve patient experiences and outcomes.
For scientists:This qualitative study recruited patients receiving buprenorphine and their prescribing physicians from two primary care-based clinics in Minnesota. Although findings here echo previous studies supporting conceptualizations of treatment success and recovery that extend beyond abstinence, future research should explore perceptions of success among a more diverse sample. Geographic, racial/ethnic, cultural, and history of treatment may all influence perceptions of success. Future studies may also explore how to effectively incorporate perceptions of success and their associated goals into treatment planning. Furthermore, identifying structural and community resources that support these goals will likely improve patient outcomes.
For policy makers: Funding and policy that helps patients accomplish their goals beyond substance use may help to improve patient engagement, treatment satisfaction, and ultimately, enhance the chances of ongoing opioid use disorder remission.