
Black Communities Hit Hardest by Lack of Public Addiction Treatment Facilities
Publicly owned outpatient substance use disorder treatment facilities are likely to accept Medicaid or offer services free of charge to vulnerable populations. However, some geographical areas have greater availability, and thus offer better access to public treatment facilities.
What are the differences between areas that offer better access versus worse access to affordable treatment options — is the racial makeup of the area an important factor to consider?
WHAT PROBLEM DOES THIS STUDY ADDRESS?
It is important that publicly funded outpatient substance use disorder treatment facilities offer services free of charge, HIV testing, and comprehensive physical and mental healthcare that is geographically accessible to vulnerable populations.
Furthermore, cross-sectional research (e.g., data from a single time point) has shown that such facilities are less likely to be located in counties with a greater percentage of black residents. Little is known about changes over time in the substance use disorder treatment infrastructure and the implications for black communities.
This study identified changes in the location of substance use disorder treatment facilities from 2002-2010 that offered outpatient treatment and classified them by ownership status (public, private nonprofit, and private for profit) because public and nonprofit facilities are less likely to turn clients away based on their ability to pay and offer vital comprehensive services.
Last, the researchers examined whether the percentage of black residents in a county was associated with changes in the availability of these outpatient facilities.
If black communities are less likely to have a supply of public or nonprofit substance use disorder treatment facilities on which they are typically dependent for adequate accessibility to substance use disorder care, it can create disparities in access to care and have important health policy implications.
HOW WAS THIS STUDY CONDUCTED?
This study merged and analyzed national data from two sources:
- The National Survey of Substance Abuse Treatment Services (N-SSATS) from 2002-2010 which is a survey of public and private facilities that provide treatment for substance use disorder
- The Health Resource Files which is a federal database of county health resources in the US and racial composition of counties. The merge yielded 3,139 counties for analysis. They identified facilities that offered outpatient treatment and classified them by ownership status (public, private nonprofit, and private for profit).
Next they determined if each county had a net gain in the number of outpatient facilities between 2002-2010, or a net loss, and if the gain or loss was associated with the racial composition of the county (e.g., percentage of black residents).
WHAT DID THIS STUDY FIND?
Between 2002 and 2010 there was a decline in the number of public and private nonprofit outpatient substance use disorder treatment facilities, but growth in the number of private for-profit facilities.
Among counties that had at least one public facility in 2002, nearly half experienced a net loss in the number of public facilities by 2010. Public facilities constituted only 15% of the sample at the beginning of the study.
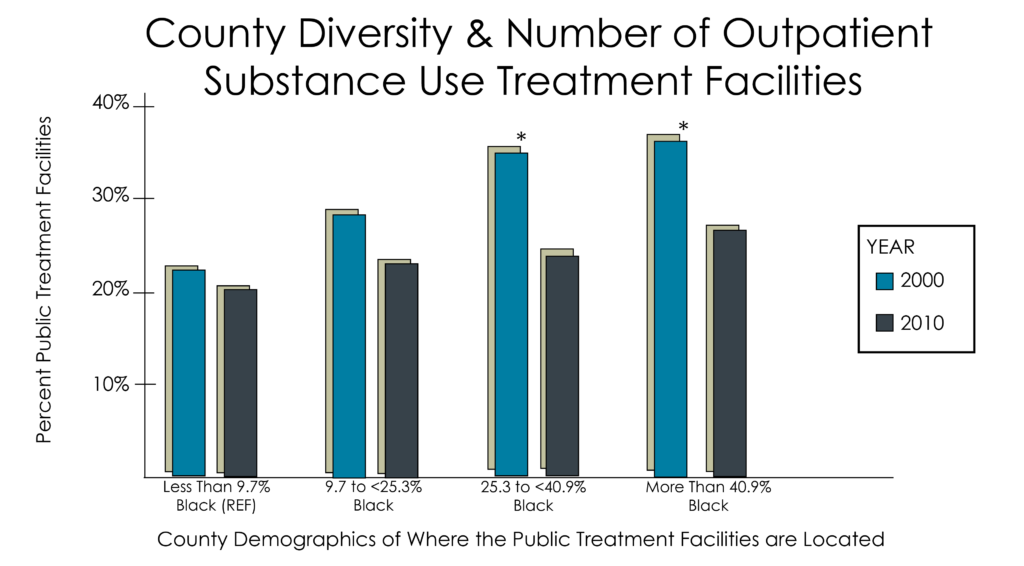
Counties with a large percentage of black residents were disproportionately burdened by the decline in public facilities, & these losses were not offset by an increased likelihood of gains in private for-profit or nonprofit facilities.
WHY IS THIS STUDY IMPORTANT?
This study highlights the importance of monitoring the geographical locations of substance use disorder treatment facilities, particularly according to ownership status and county demographics (e.g., racial composition) for equivalent access to care.
The decline in public substance use disorder facilitates for black communities has not been offset by an increase in private for profit or nonprofit facilities. This means that counties with high proportions of black residents are less likely to have geographical access to vital, affordable treatment resources.
Given the body of research that has shown the beneficial effects of treatment on reducing substance use disorder, unequal access to care can create health disparities in recovery from substance use disorder.
It is important to note, that the statistical analysis (e.g., regression) indicated there was no significant association between county percentage of black residents and the likelihood of losing a public facility after adjusting for other county-level characteristics. This means that although counties with higher proportions of black residents were disproportionately affected by the decline in public substance use disorder facilities, racial composition doesn’t “explain” the variance over and above other county-level characteristics.
In other words, we cannot conclude that race itself is responsible for the decline in public substance use disorder facilities, it is possible the other factors correlated with race, such as the economic condition of the county are also associated with the net loss of public substance use treatment facilities.
- LIMITATIONS
-
- One limitation is that the unit of analysis was measured on the county level, not individual. Therefore, we do not know if the decline in public substance use disorder treatment facilities in counties with high proportions of black residents is a detriment to individuals with substance use disorder or their treatment and recovery outcomes.
NEXT STEPS
The county is a meaningful unit of analysis for health resource planning purposes and has been used to understand the distribution of outpatient health care resources for vulnerable populations; however, county sizes can vary considerably.
Future research should examine the availability of facilities using a more sensitive unit of analysis as data become available so a more direct inference can be made between the proportion of vulnerable residents (e.g., impoverished) and geographical access to substance use disorder treatment in a way that more closely mirrors their proximal geographical context. Specifically, the census-tract level of analysis has been shown to be particularly sensitive to socioeconomic gradients.
BOTTOM LINE
- For individuals & families seeking recovery: If you or a family member are in need of treatment for a substance use disorder, the availability of public treatment facilities may have substantially declined in your county. Consider seeking treatment at a private for profit or private nonprofit treatment facility if a public facility is not available. Despite having disproportionate increases in counties with more nonblack residents, for profit facilities are another source of treatment availability.
- For Scientists: More work is needed to establish the role that treatment availability and ownership type (for profit vs. public not for profit) have on treatment and recovery. Importantly, establishing if the relationship between treatment availability and treatment or recovery outcomes is the same in all counties can have important health policy implications.
- For Policy makers: There are gaps in the substance use disorder treatment infrastructure for black communities that resulted from the closure of public or private nonprofit facilities. Allocation of resources to provide monitoring and surveillance of changes in the treatment infrastructure, particularly for vulnerable communities, could help prevent the creation of treatment system gaps. The disproportionate availability of treatment services has the potential to recreate health disparities.
- For Treatment professionals and treatment systems: If you work at a private for-profit or private nonprofit substance use disorder treatment facility in a county with many black residents, consider accepting Medicaid, offering free services, or more comprehensive services (e.g., HIV testing, mental healthcare, etc.) to offset a potential lack of access to care normally offered by public nonprofit substance use disorder facilities.
CITATIONS
Cummings, J.R., Wen, H., & Ko, M. (2016). Decline in public substance use disorder treatment centers most serious in counties with high shares of black residents. Health Affairs, 35. 1036-1044