Can a web-based intervention help spouses of heavy drinkers?
The consequences of heavy and harmful alcohol use can be emotionally and psychologically impactful – not just for the person consuming alcohol, but also for their loved ones who often lack specific knowledge and support. This study tested a novel web-based intervention for supporting military spouses adapted from an established intervention for concerned significant others of individuals with substance use disorder.
While CRAFT appears to be a helpful intervention, finding CRAFT trained clinicians can be challenging. Additionally, military families may experience stigma around seeking psychological support for substance use issues due to a culture of masculinity that shuns perceived weakness, making military personnel and their concerned significant others less likely to engage in this and other kinds of psychological care. To offset these barriers to help seeking, the researchers in this study developed a web-based version of CRAFT to specifically address the needs of military spouses—referred to here as concerned partners—condensing the usual 12 in-person sessions into 4 online modules.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized, waitlist controlled clinical trial with 234 concerned partners who received either four sessions of web-based CRAFT aimed at improving psychological health and communication skills, or no intervention.
The web-based CRAFT intervention, called “Partners Connect” included the following material delivered across the four sessions: 1) Concerned partners received personalized feedback about their own drinking and mental health issues and were encouraged to engage in pleasant activities for self-care and identify a support person to talk with about their concerns. They were also encouraged to practice skills with their social support person in-between sessions. 2) Positive communication skills training was provided, as were skills to reinforce their partner’s sobriety. 3) Skills training was also provided around cultivating self-care and talking with identified patients about their concerns, while interacting with their partner in healthy ways.
Though this online version of CRAFT focused less on behavior change skills designed to get loved ones into addiction treatment, the researchers surmised that improved communication over time would still help partners misusing alcohol—referred to here as the identified patient—to reduce their drinking and seek care.
Each module was 30-45 minutes in length, and included, 1) a video introducing the class’s topic; 2) interactive questions and personalized feedback based on concerned partners’ baseline or between-session survey responses, 3) instruction in skills building, and 4) a description of next steps. Classes were spaced one week apart to give concerned partners a chance to practice the skills learned in the prior session. If they did not finish a session, they could continue from where they left off later.
The randomized study sample included 136 concerned partners who received web-based CRAFT, and 98 who received the waitlist condition (the control group). Of the full sample, 95% of participants were female, 71% were White, 9% multi-racial, 6% African American, and 4% Hispanic/Latino. Participants were on average 32 years of age. About 89% of concerned partners were married to their spouse and 77% had children.
The outcomes measured at baseline and at 5 months post-treatment included the concerned partners’ levels of 1) depression, 2) anxiety, 3) anger expression, 4) social support, 5) relationship quality, 6) family conflict, and 7) their own alcohol use. The researchers also asked concerned partners to estimate their partner’s alcohol use.
Study eligibility criteria included being 18+ years of age and indicating at least a value of ‘3’ on scale from “1 not at all” to “7 very much” for the degree to which they felt their partner had an alcohol problem.
WHAT DID THIS STUDY FIND?
Military spouses had elevated anxiety and depression.
At baseline assessment, approximately half the study sample (54.7%) of concerned partners experienced major depression, generalized anxiety disorder, or heavy drinking episodes. Of these individuals, 63% had not received any therapy or attended a mutual-help organization in the past year.
Most concerned partners (88%) stated that their identified patient partners drank heavily (five drinks or more per drinking occasion) at least once in the past month and drank an average of 10 drinks on their heaviest drinking occasion in the past month.
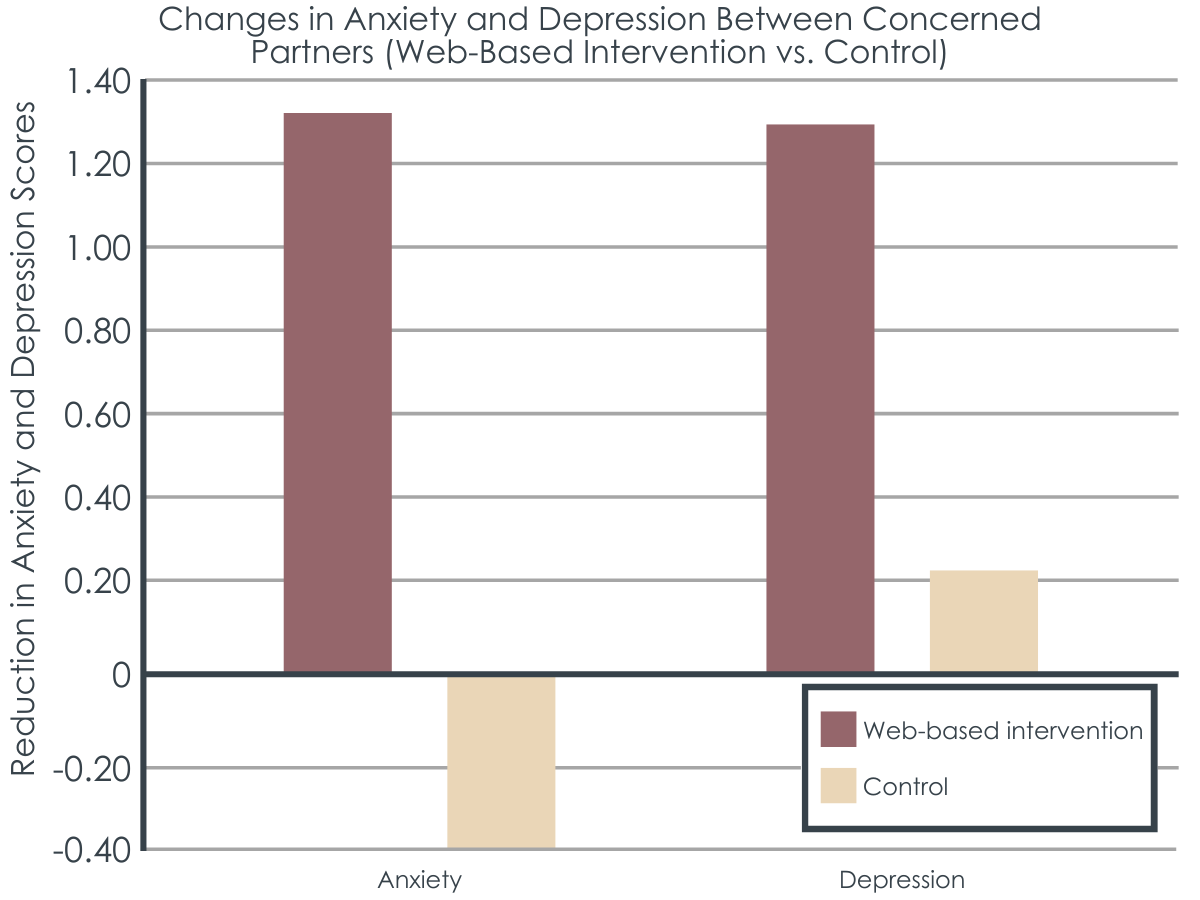
Figure 2. Changes in scores of anxiety and depression from baseline to X months were reported for both intervention and control groups. Positive numbers indicate a reduction in anxiety and depression (i.e., an increase in the reduction), while negative numbers indicate that anxiety and depression increased.
The intervention group improved their psychological health, albeit slightly.
The web-based CRAFT group had less anxiety and greater informational and tangible social support at follow-up compared to controls who did not receive the intervention. At the same time, the observed differences were not large. For instance, participants receiving CRAFT reported an average reduction of 1.32 points on the researchers’ measure of anxiety (the 7-item Generalized Anxiety Disorder questionnaire best known by the acronym GAD-7), while controls reported a symptom increase of 0.4. Given the GAD-7 questionnaire has a range of 0-21, this advantage may not reflect a clinically meaningful difference.
There were no observed intervention effects on depression, anger expression, relationship quality, family conflict, or positive social interaction support, nor was there an observed effect on perceived identified patient drinking over time.
As is often the case with intervention outcome evaluations, individuals who completed more modules had greater reductions in anxiety, depression, and anger expression, as well as greater increases in tangible social support and positive social interactions. Overall, in the CRAFT group, 13% of participants did not complete any sessions, 11% completed one, 4% completed two, 7% completed three, and 65% completed all four web-based sessions.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
CRAFT has been shown to help concerned significant others (referred to here as concerned partners) better care for themselves while trying to cope with a loved one’s hazardous drinking and get their loved ones into treatment sooner.
Questions remain however about the effectiveness of adapted, online versions of CRAFT that are delivered with little or no clinician support. A recent clinical trial showed that a condensed, five-session CRAFT intervention with offline clinician coaching helped improve concerned significant others’ psychological well-being, however, treatment effects were not sustained at 6, 12, or 24-week follow-up.
Here, researchers tested a four-module, adapted online CRAFT intervention that did not include provider contact. Though the group receiving the intervention did better than controls in terms of slight reductions in anxiety and improvements in tangible and informational social support, these differences represented small effect sizes, and may not reflect clinically meaningful treatment effects.
Notably, the authors did find a dose effect, such that participants completing a greater number of the four online CRAFT session had greater reductions in anxiety, depression, and anger expression from study baseline to 5-month follow-up. This may represent an effect of the intervention but may also be an artifact of participants with greater intrinsic motivation to change also completing more treatment sessions. In other words, these participants may have improved not because they did more CRAFT sessions, but because they were more motivated to change and were seeking other forms of support not measured in this study.
The researchers controlled for effects of children in their statistical analyses. Notably, after accounting for other demographic factors, having children was associated with greater anxiety and depression in the concerned partners. This highlights an additional burden that partners of military personnel may face who also have children to raise and care for. Future iterations of CRAFT-based interventions for this population may do well to include a component on managing the additional burdens of being a parent in the training modules.
This study was also notable for its high attrition rate with 27.8% of CRAFT group participants, and 18.0% of waitlist control group participants lost to follow-up. The higher attrition rate in the CRAFT group may be a function of dissatisfaction with the intervention, or failures of the intervention to help participants. Ideally, future studies will use intent-to-treat analysis (a method that assumes study non-completers had a bad treatment outcome) to account for attrition in their final results.
The study sample consisted of mostly young, White women who were married to male military personnel. Future studies will ideally test web-based CRAFT interventions for concerned military partners with more diverse samples.
The training vignettes used in the online classes in this study were limited to vignettes about female concerned partners and did not account for male concerned partners’ perspectives or same-sex relationships. Ideally, future iterations of this intervention will allow adaption of these training vignettes to match the gender and sexual orientation of concerned partners.
Concerned partners may have over- or under-estimated their partner’s drinking. Ideally future studies will include objective measures of both concerned partner and identified patient drinking.
Many participants were lost to follow-up (72 of 312). It is hard to know how this may have inadvertently affected study outcomes.
BOTTOM LINE
Previous research has shown that Community Reinforcement Approach and Family Training (CRAFT) can increase the well-being of concerned significant others and help identified patients reduce their substance use and engage with treatment sooner. Though the abbreviated, web-based version of CRAFT for military spouses tested in this study appeared to produce some benefits, the observed effect sizes were small, and the groups did not differ ona number ofstudy measures.That being said, with further development and testing, this web-based CRAFT intervention could still prove useful to military spouses with partners misusing alcohol.Qualitative assessment would have been helpful in this study in order to understand more about what these spouses liked/didn’t like about the intervention,the barriers to completing the sessions, and how the procedure and contents might be improved to better meet their needs, or whether new types of interventions should be developed. This kind of information could prove indispensable in better helping concerned significant others through online web-based self-help formats.
For individuals and families seeking recovery: More development and testing is needed before a condensed, web-based CRAFT intervention is ready for widescale dissemination to military spouses. At the same time, previous studies have shown that provider-delivered CRAFT works quite well in terms of improving the well-being of concerned significant others and getting identified patients into treatment sooner. While finding a provider trained to deliver CRAFT can be challenging, with the mainstreaming of telehealth during the COVID-19 pandemic, it’s increasingly possible to find providers outside of one’s hometown who can provide this service.
For treatment professionals and treatment systems: More development and testing is needed before a condensed, web-based CRAFT intervention is ready for widescale dissemination to military spouses. At the same time, previous studies have shown that provider-delivered CRAFT works well in terms of improving the well-being of concerned significant others and getting identified patients into treatment sooner. Moreover, CRAFT provides an important, more potent alternative to traditional confrontational approaches such as the family “intervention”.
For scientists:A condensed, web-based CRAFT intervention for military spouses with partners who drink alcohol in harmful and hazardous ways could help many access care where they would otherwise receive none. The web-based CRAFT adaptation used in this study has promise, but more quantitative and qualitative research is needed to help inform, develop, and test this intervention.
For policy makers: The web-based version of CRAFT tested in this study will require additional development and testing before it’s ready for wide-scale dissemination. Until then, traditional, provider-delivered CRAFT remains an important tool for supporting concerned significant others and helping them get their loved ones into addiction treatment sooner. Policies that require insurance providers to reimburse for CRAFT will indirectly improve public health and save healthcare systems by improving the psychological well-being of concerned significant others and getting people with substance use disorder into treatment faster.
While CRAFT appears to be a helpful intervention, finding CRAFT trained clinicians can be challenging. Additionally, military families may experience stigma around seeking psychological support for substance use issues due to a culture of masculinity that shuns perceived weakness, making military personnel and their concerned significant others less likely to engage in this and other kinds of psychological care. To offset these barriers to help seeking, the researchers in this study developed a web-based version of CRAFT to specifically address the needs of military spouses—referred to here as concerned partners—condensing the usual 12 in-person sessions into 4 online modules.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized, waitlist controlled clinical trial with 234 concerned partners who received either four sessions of web-based CRAFT aimed at improving psychological health and communication skills, or no intervention.
The web-based CRAFT intervention, called “Partners Connect” included the following material delivered across the four sessions: 1) Concerned partners received personalized feedback about their own drinking and mental health issues and were encouraged to engage in pleasant activities for self-care and identify a support person to talk with about their concerns. They were also encouraged to practice skills with their social support person in-between sessions. 2) Positive communication skills training was provided, as were skills to reinforce their partner’s sobriety. 3) Skills training was also provided around cultivating self-care and talking with identified patients about their concerns, while interacting with their partner in healthy ways.
Though this online version of CRAFT focused less on behavior change skills designed to get loved ones into addiction treatment, the researchers surmised that improved communication over time would still help partners misusing alcohol—referred to here as the identified patient—to reduce their drinking and seek care.
Each module was 30-45 minutes in length, and included, 1) a video introducing the class’s topic; 2) interactive questions and personalized feedback based on concerned partners’ baseline or between-session survey responses, 3) instruction in skills building, and 4) a description of next steps. Classes were spaced one week apart to give concerned partners a chance to practice the skills learned in the prior session. If they did not finish a session, they could continue from where they left off later.
The randomized study sample included 136 concerned partners who received web-based CRAFT, and 98 who received the waitlist condition (the control group). Of the full sample, 95% of participants were female, 71% were White, 9% multi-racial, 6% African American, and 4% Hispanic/Latino. Participants were on average 32 years of age. About 89% of concerned partners were married to their spouse and 77% had children.
The outcomes measured at baseline and at 5 months post-treatment included the concerned partners’ levels of 1) depression, 2) anxiety, 3) anger expression, 4) social support, 5) relationship quality, 6) family conflict, and 7) their own alcohol use. The researchers also asked concerned partners to estimate their partner’s alcohol use.
Study eligibility criteria included being 18+ years of age and indicating at least a value of ‘3’ on scale from “1 not at all” to “7 very much” for the degree to which they felt their partner had an alcohol problem.
WHAT DID THIS STUDY FIND?
Military spouses had elevated anxiety and depression.
At baseline assessment, approximately half the study sample (54.7%) of concerned partners experienced major depression, generalized anxiety disorder, or heavy drinking episodes. Of these individuals, 63% had not received any therapy or attended a mutual-help organization in the past year.
Most concerned partners (88%) stated that their identified patient partners drank heavily (five drinks or more per drinking occasion) at least once in the past month and drank an average of 10 drinks on their heaviest drinking occasion in the past month.
Figure 2. Changes in scores of anxiety and depression from baseline to X months were reported for both intervention and control groups. Positive numbers indicate a reduction in anxiety and depression (i.e., an increase in the reduction), while negative numbers indicate that anxiety and depression increased.
The intervention group improved their psychological health, albeit slightly.
The web-based CRAFT group had less anxiety and greater informational and tangible social support at follow-up compared to controls who did not receive the intervention. At the same time, the observed differences were not large. For instance, participants receiving CRAFT reported an average reduction of 1.32 points on the researchers’ measure of anxiety (the 7-item Generalized Anxiety Disorder questionnaire best known by the acronym GAD-7), while controls reported a symptom increase of 0.4. Given the GAD-7 questionnaire has a range of 0-21, this advantage may not reflect a clinically meaningful difference.
There were no observed intervention effects on depression, anger expression, relationship quality, family conflict, or positive social interaction support, nor was there an observed effect on perceived identified patient drinking over time.
As is often the case with intervention outcome evaluations, individuals who completed more modules had greater reductions in anxiety, depression, and anger expression, as well as greater increases in tangible social support and positive social interactions. Overall, in the CRAFT group, 13% of participants did not complete any sessions, 11% completed one, 4% completed two, 7% completed three, and 65% completed all four web-based sessions.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
CRAFT has been shown to help concerned significant others (referred to here as concerned partners) better care for themselves while trying to cope with a loved one’s hazardous drinking and get their loved ones into treatment sooner.
Questions remain however about the effectiveness of adapted, online versions of CRAFT that are delivered with little or no clinician support. A recent clinical trial showed that a condensed, five-session CRAFT intervention with offline clinician coaching helped improve concerned significant others’ psychological well-being, however, treatment effects were not sustained at 6, 12, or 24-week follow-up.
Here, researchers tested a four-module, adapted online CRAFT intervention that did not include provider contact. Though the group receiving the intervention did better than controls in terms of slight reductions in anxiety and improvements in tangible and informational social support, these differences represented small effect sizes, and may not reflect clinically meaningful treatment effects.
Notably, the authors did find a dose effect, such that participants completing a greater number of the four online CRAFT session had greater reductions in anxiety, depression, and anger expression from study baseline to 5-month follow-up. This may represent an effect of the intervention but may also be an artifact of participants with greater intrinsic motivation to change also completing more treatment sessions. In other words, these participants may have improved not because they did more CRAFT sessions, but because they were more motivated to change and were seeking other forms of support not measured in this study.
The researchers controlled for effects of children in their statistical analyses. Notably, after accounting for other demographic factors, having children was associated with greater anxiety and depression in the concerned partners. This highlights an additional burden that partners of military personnel may face who also have children to raise and care for. Future iterations of CRAFT-based interventions for this population may do well to include a component on managing the additional burdens of being a parent in the training modules.
This study was also notable for its high attrition rate with 27.8% of CRAFT group participants, and 18.0% of waitlist control group participants lost to follow-up. The higher attrition rate in the CRAFT group may be a function of dissatisfaction with the intervention, or failures of the intervention to help participants. Ideally, future studies will use intent-to-treat analysis (a method that assumes study non-completers had a bad treatment outcome) to account for attrition in their final results.
The study sample consisted of mostly young, White women who were married to male military personnel. Future studies will ideally test web-based CRAFT interventions for concerned military partners with more diverse samples.
The training vignettes used in the online classes in this study were limited to vignettes about female concerned partners and did not account for male concerned partners’ perspectives or same-sex relationships. Ideally, future iterations of this intervention will allow adaption of these training vignettes to match the gender and sexual orientation of concerned partners.
Concerned partners may have over- or under-estimated their partner’s drinking. Ideally future studies will include objective measures of both concerned partner and identified patient drinking.
Many participants were lost to follow-up (72 of 312). It is hard to know how this may have inadvertently affected study outcomes.
BOTTOM LINE
Previous research has shown that Community Reinforcement Approach and Family Training (CRAFT) can increase the well-being of concerned significant others and help identified patients reduce their substance use and engage with treatment sooner. Though the abbreviated, web-based version of CRAFT for military spouses tested in this study appeared to produce some benefits, the observed effect sizes were small, and the groups did not differ ona number ofstudy measures.That being said, with further development and testing, this web-based CRAFT intervention could still prove useful to military spouses with partners misusing alcohol.Qualitative assessment would have been helpful in this study in order to understand more about what these spouses liked/didn’t like about the intervention,the barriers to completing the sessions, and how the procedure and contents might be improved to better meet their needs, or whether new types of interventions should be developed. This kind of information could prove indispensable in better helping concerned significant others through online web-based self-help formats.
For individuals and families seeking recovery: More development and testing is needed before a condensed, web-based CRAFT intervention is ready for widescale dissemination to military spouses. At the same time, previous studies have shown that provider-delivered CRAFT works quite well in terms of improving the well-being of concerned significant others and getting identified patients into treatment sooner. While finding a provider trained to deliver CRAFT can be challenging, with the mainstreaming of telehealth during the COVID-19 pandemic, it’s increasingly possible to find providers outside of one’s hometown who can provide this service.
For treatment professionals and treatment systems: More development and testing is needed before a condensed, web-based CRAFT intervention is ready for widescale dissemination to military spouses. At the same time, previous studies have shown that provider-delivered CRAFT works well in terms of improving the well-being of concerned significant others and getting identified patients into treatment sooner. Moreover, CRAFT provides an important, more potent alternative to traditional confrontational approaches such as the family “intervention”.
For scientists:A condensed, web-based CRAFT intervention for military spouses with partners who drink alcohol in harmful and hazardous ways could help many access care where they would otherwise receive none. The web-based CRAFT adaptation used in this study has promise, but more quantitative and qualitative research is needed to help inform, develop, and test this intervention.
For policy makers: The web-based version of CRAFT tested in this study will require additional development and testing before it’s ready for wide-scale dissemination. Until then, traditional, provider-delivered CRAFT remains an important tool for supporting concerned significant others and helping them get their loved ones into addiction treatment sooner. Policies that require insurance providers to reimburse for CRAFT will indirectly improve public health and save healthcare systems by improving the psychological well-being of concerned significant others and getting people with substance use disorder into treatment faster.
While CRAFT appears to be a helpful intervention, finding CRAFT trained clinicians can be challenging. Additionally, military families may experience stigma around seeking psychological support for substance use issues due to a culture of masculinity that shuns perceived weakness, making military personnel and their concerned significant others less likely to engage in this and other kinds of psychological care. To offset these barriers to help seeking, the researchers in this study developed a web-based version of CRAFT to specifically address the needs of military spouses—referred to here as concerned partners—condensing the usual 12 in-person sessions into 4 online modules.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized, waitlist controlled clinical trial with 234 concerned partners who received either four sessions of web-based CRAFT aimed at improving psychological health and communication skills, or no intervention.
The web-based CRAFT intervention, called “Partners Connect” included the following material delivered across the four sessions: 1) Concerned partners received personalized feedback about their own drinking and mental health issues and were encouraged to engage in pleasant activities for self-care and identify a support person to talk with about their concerns. They were also encouraged to practice skills with their social support person in-between sessions. 2) Positive communication skills training was provided, as were skills to reinforce their partner’s sobriety. 3) Skills training was also provided around cultivating self-care and talking with identified patients about their concerns, while interacting with their partner in healthy ways.
Though this online version of CRAFT focused less on behavior change skills designed to get loved ones into addiction treatment, the researchers surmised that improved communication over time would still help partners misusing alcohol—referred to here as the identified patient—to reduce their drinking and seek care.
Each module was 30-45 minutes in length, and included, 1) a video introducing the class’s topic; 2) interactive questions and personalized feedback based on concerned partners’ baseline or between-session survey responses, 3) instruction in skills building, and 4) a description of next steps. Classes were spaced one week apart to give concerned partners a chance to practice the skills learned in the prior session. If they did not finish a session, they could continue from where they left off later.
The randomized study sample included 136 concerned partners who received web-based CRAFT, and 98 who received the waitlist condition (the control group). Of the full sample, 95% of participants were female, 71% were White, 9% multi-racial, 6% African American, and 4% Hispanic/Latino. Participants were on average 32 years of age. About 89% of concerned partners were married to their spouse and 77% had children.
The outcomes measured at baseline and at 5 months post-treatment included the concerned partners’ levels of 1) depression, 2) anxiety, 3) anger expression, 4) social support, 5) relationship quality, 6) family conflict, and 7) their own alcohol use. The researchers also asked concerned partners to estimate their partner’s alcohol use.
Study eligibility criteria included being 18+ years of age and indicating at least a value of ‘3’ on scale from “1 not at all” to “7 very much” for the degree to which they felt their partner had an alcohol problem.
WHAT DID THIS STUDY FIND?
Military spouses had elevated anxiety and depression.
At baseline assessment, approximately half the study sample (54.7%) of concerned partners experienced major depression, generalized anxiety disorder, or heavy drinking episodes. Of these individuals, 63% had not received any therapy or attended a mutual-help organization in the past year.
Most concerned partners (88%) stated that their identified patient partners drank heavily (five drinks or more per drinking occasion) at least once in the past month and drank an average of 10 drinks on their heaviest drinking occasion in the past month.
Figure 2. Changes in scores of anxiety and depression from baseline to X months were reported for both intervention and control groups. Positive numbers indicate a reduction in anxiety and depression (i.e., an increase in the reduction), while negative numbers indicate that anxiety and depression increased.
The intervention group improved their psychological health, albeit slightly.
The web-based CRAFT group had less anxiety and greater informational and tangible social support at follow-up compared to controls who did not receive the intervention. At the same time, the observed differences were not large. For instance, participants receiving CRAFT reported an average reduction of 1.32 points on the researchers’ measure of anxiety (the 7-item Generalized Anxiety Disorder questionnaire best known by the acronym GAD-7), while controls reported a symptom increase of 0.4. Given the GAD-7 questionnaire has a range of 0-21, this advantage may not reflect a clinically meaningful difference.
There were no observed intervention effects on depression, anger expression, relationship quality, family conflict, or positive social interaction support, nor was there an observed effect on perceived identified patient drinking over time.
As is often the case with intervention outcome evaluations, individuals who completed more modules had greater reductions in anxiety, depression, and anger expression, as well as greater increases in tangible social support and positive social interactions. Overall, in the CRAFT group, 13% of participants did not complete any sessions, 11% completed one, 4% completed two, 7% completed three, and 65% completed all four web-based sessions.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
CRAFT has been shown to help concerned significant others (referred to here as concerned partners) better care for themselves while trying to cope with a loved one’s hazardous drinking and get their loved ones into treatment sooner.
Questions remain however about the effectiveness of adapted, online versions of CRAFT that are delivered with little or no clinician support. A recent clinical trial showed that a condensed, five-session CRAFT intervention with offline clinician coaching helped improve concerned significant others’ psychological well-being, however, treatment effects were not sustained at 6, 12, or 24-week follow-up.
Here, researchers tested a four-module, adapted online CRAFT intervention that did not include provider contact. Though the group receiving the intervention did better than controls in terms of slight reductions in anxiety and improvements in tangible and informational social support, these differences represented small effect sizes, and may not reflect clinically meaningful treatment effects.
Notably, the authors did find a dose effect, such that participants completing a greater number of the four online CRAFT session had greater reductions in anxiety, depression, and anger expression from study baseline to 5-month follow-up. This may represent an effect of the intervention but may also be an artifact of participants with greater intrinsic motivation to change also completing more treatment sessions. In other words, these participants may have improved not because they did more CRAFT sessions, but because they were more motivated to change and were seeking other forms of support not measured in this study.
The researchers controlled for effects of children in their statistical analyses. Notably, after accounting for other demographic factors, having children was associated with greater anxiety and depression in the concerned partners. This highlights an additional burden that partners of military personnel may face who also have children to raise and care for. Future iterations of CRAFT-based interventions for this population may do well to include a component on managing the additional burdens of being a parent in the training modules.
This study was also notable for its high attrition rate with 27.8% of CRAFT group participants, and 18.0% of waitlist control group participants lost to follow-up. The higher attrition rate in the CRAFT group may be a function of dissatisfaction with the intervention, or failures of the intervention to help participants. Ideally, future studies will use intent-to-treat analysis (a method that assumes study non-completers had a bad treatment outcome) to account for attrition in their final results.
The study sample consisted of mostly young, White women who were married to male military personnel. Future studies will ideally test web-based CRAFT interventions for concerned military partners with more diverse samples.
The training vignettes used in the online classes in this study were limited to vignettes about female concerned partners and did not account for male concerned partners’ perspectives or same-sex relationships. Ideally, future iterations of this intervention will allow adaption of these training vignettes to match the gender and sexual orientation of concerned partners.
Concerned partners may have over- or under-estimated their partner’s drinking. Ideally future studies will include objective measures of both concerned partner and identified patient drinking.
Many participants were lost to follow-up (72 of 312). It is hard to know how this may have inadvertently affected study outcomes.
BOTTOM LINE
Previous research has shown that Community Reinforcement Approach and Family Training (CRAFT) can increase the well-being of concerned significant others and help identified patients reduce their substance use and engage with treatment sooner. Though the abbreviated, web-based version of CRAFT for military spouses tested in this study appeared to produce some benefits, the observed effect sizes were small, and the groups did not differ ona number ofstudy measures.That being said, with further development and testing, this web-based CRAFT intervention could still prove useful to military spouses with partners misusing alcohol.Qualitative assessment would have been helpful in this study in order to understand more about what these spouses liked/didn’t like about the intervention,the barriers to completing the sessions, and how the procedure and contents might be improved to better meet their needs, or whether new types of interventions should be developed. This kind of information could prove indispensable in better helping concerned significant others through online web-based self-help formats.
For individuals and families seeking recovery: More development and testing is needed before a condensed, web-based CRAFT intervention is ready for widescale dissemination to military spouses. At the same time, previous studies have shown that provider-delivered CRAFT works quite well in terms of improving the well-being of concerned significant others and getting identified patients into treatment sooner. While finding a provider trained to deliver CRAFT can be challenging, with the mainstreaming of telehealth during the COVID-19 pandemic, it’s increasingly possible to find providers outside of one’s hometown who can provide this service.
For treatment professionals and treatment systems: More development and testing is needed before a condensed, web-based CRAFT intervention is ready for widescale dissemination to military spouses. At the same time, previous studies have shown that provider-delivered CRAFT works well in terms of improving the well-being of concerned significant others and getting identified patients into treatment sooner. Moreover, CRAFT provides an important, more potent alternative to traditional confrontational approaches such as the family “intervention”.
For scientists:A condensed, web-based CRAFT intervention for military spouses with partners who drink alcohol in harmful and hazardous ways could help many access care where they would otherwise receive none. The web-based CRAFT adaptation used in this study has promise, but more quantitative and qualitative research is needed to help inform, develop, and test this intervention.
For policy makers: The web-based version of CRAFT tested in this study will require additional development and testing before it’s ready for wide-scale dissemination. Until then, traditional, provider-delivered CRAFT remains an important tool for supporting concerned significant others and helping them get their loved ones into addiction treatment sooner. Policies that require insurance providers to reimburse for CRAFT will indirectly improve public health and save healthcare systems by improving the psychological well-being of concerned significant others and getting people with substance use disorder into treatment faster.