Can a web-based intervention help family members get their loved one into substance use disorder treatment sooner?
Community Reinforcement Approach and Family Training (CRAFT) is an intervention for concerned significant others of individuals with substance use problems designed to get loved ones into treatment while improving their own well-being. Yet this type of help for concerned and affected family members can be hard to find with few clinicians trained in this approach. This study developed and tested an web-based version of CRAFT that does not require a clinician to deliver it, which, if shown to be helpful, has the potential to reach many more people.
Engaging individuals in substance use disorder treatment can be incredibly challenging. Community Reinforcement Approach and Family Training (known by the acronym CRAFT) is a relatively brief intervention designed to help loved ones of people with substance use disorder get their loved one to reduce or stop their substance use, engage with treatment, while better caring for themselves. CRAFT is usually delivered over the course of 10-12 therapy sessions with a trained provider. What makes CRAFT unique is that it engages the concerned significant other/s without directly engaging the identified patient (also referred to as the concerned significant other’s “loved one”). The intervention is largely based on established principles of behavioral psychology, which can be used to shape behavior change, mostly by providing or withdrawing different types of natural rewards in the home environment (e.g., rewarding pro-recovery behaviors; withdrawing attention when substance use persists).
To increase access to CRAFT, the researchers in this study developed an internet-delivered version, which condensed clinician-delivered CRAFT into 5 brief video modules along with some online training materials. In this internet-delivered version of CRAFT, participants complete online worksheets during classes, as well as related homework assignments, which are independently reviewed by a CRAFT trained provider, who later provides written feedback through the online portal. There was no live-time (i.e., “synchronous”) communication between patients and providers.
The researchers tested their internet-delivered version of CRAFT in a controlled trial to determine whether this intervention would produce similar outcomes to previous clinical trials of traditional, clinician-delivered CRAFT.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized, waitlist-controlled trial with 94 concerned significant others with a treatment-reluctant loved one with alcohol use disorder (based on the concerned significant other’s report). Participants received 5 online sessions of CRAFT with asynchronous online support from a CRAFT trained clinician or were randomized to a waitlist-control group. All participants, recruited nationwide in Sweden, were assessed at study baseline, and then again at 6, 12, and 24-weeks after entering the study.
The internet-delivered CRAFT intervention included, 1) An overview of CRAFT’s structure designed to bolster concerned significant other’s motivation to engage with the intervention, 2) self-care strategies to help concerned significant others improve their own well-being, 3) strategies designed to maximize the likelihood the identified patient will seek treatment when asked, 4) communication skills, and 5) behavioral reinforcement skills. Click here for a more detailed description of the CRAFT intervention.
Each session included a combination of short video clips, exercises designed to help the concerned significant others learn new skills, and homework assignments to practice these skills. Participants’ responses to the session exercises and their homework assignments were reported in text to a study therapist through the researchers’ CRAFT platform. The therapist gave written feedback on their own time (i.e., asynchronously) based on the established CRAFT protocol through the internet-based CRAFT system. There was no live-time (i.e., synchronous) in-person contact between participants and study therapists. Although the active treatment period lasted 5 weeks, participants had access to web-based CRAFT for the entire 24-week study period.
Participants randomized to the waitlist control group received the same assessments as participants randomized to receive internet-based CRAFT but were only invited to receive the intervention after completing the study. For the purposes of this study, the waitlist condition was equivalent to an assessment-only comparison group.
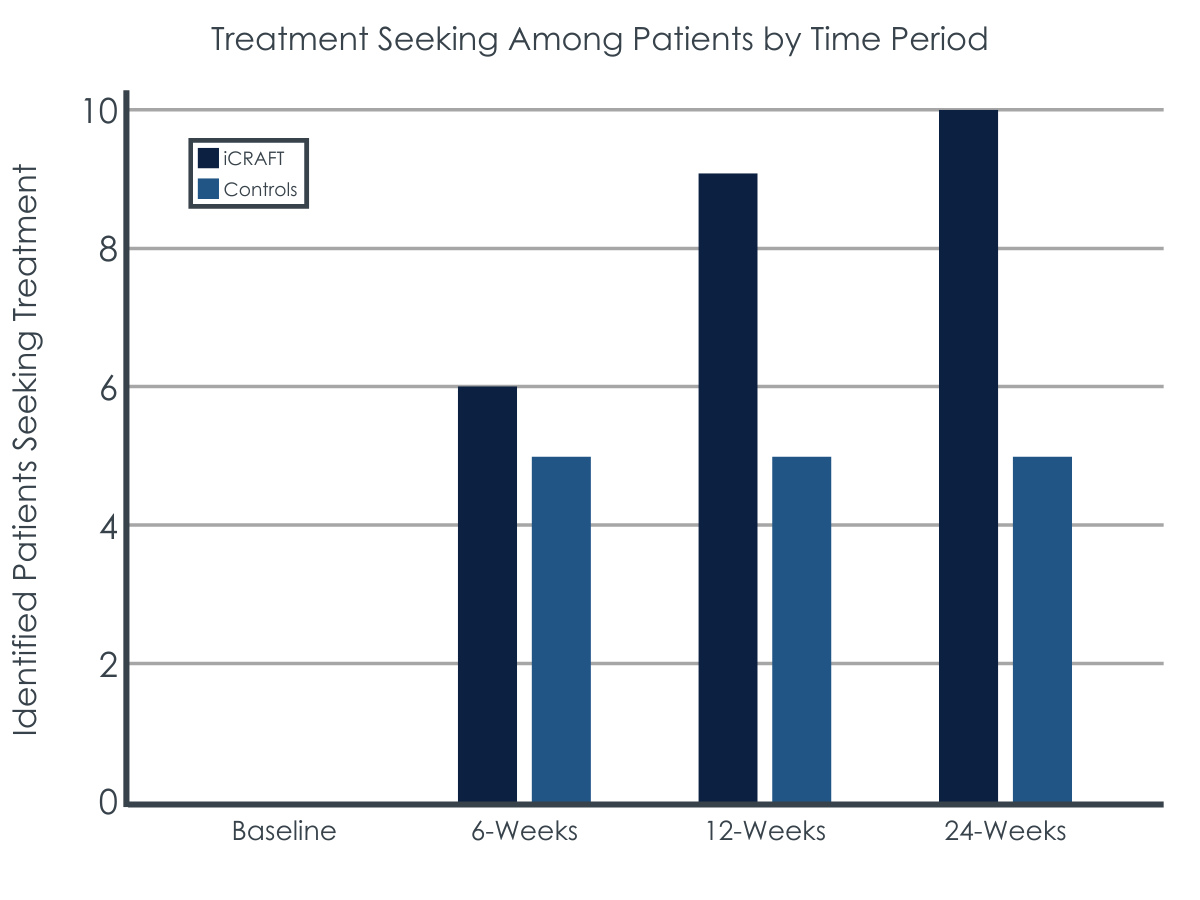
The main study outcome was the proportion of identified patients seeking treatment for substance use disorder over the course of the 24-week follow-up period. Secondary outcomes included change in identified patients’ alcohol use from baseline to 6, 12 and 24-week follow-up, concerned significant others’ depression, anxiety, stress, and well-being, as well as their relational satisfaction with the identified patient.
Inclusion criteria for concerned significant others were: 1) Having an ongoing relationship with a treatment resistant identified patient meeting the Diagnostic and Statistical Manual of Mental Disorders IV (commonly referred to as DSM-IV) diagnosis of alcohol dependence or abuse based on diagnostic information provided by the participant (not the identified patient), 2) being at least 18 years of age, 3) spending significant time with the identified patient, defined as greater than 40% of the last 90 days, 4) confirmation from the concerned significant other that their identified patient had consumed alcohol in at least 30 of the past 90 days, and 5) having a goal of engaging the identified patient in treatment.
Exclusion criteria were: 1) Identified patients not being treatment resistant [i.e. they would seek treatment if asked], 2) identified patients receiving alcohol-related treatment within the past 6 months, 3) major psychiatric or physical illness in the concerned significant other or identified patient, 4) the identified patient having a DSM-IV diagnosis of substance dependence or abuse [not including alcohol or nicotine], 5) insufficient Swedish language comprehension, 6) participation in a concerned significant other mutual-support program like Al-Anon in the past 12 months, and 7) risk for domestic violence by the identified patient.
WHAT DID THIS STUDY FIND?
Participants were mostly female and in a partner relationship with the identified patient.
Almost all study participants identified as female (97.9%) and 86.2% were in a partner relationship with the identified patient. Concerned significant others randomized to the internet-based CRAFT group completed on average 3 of the 5 CRAFT online sessions. Per participant report, identified patients consumed an average of 5.4 drinks per day on 4.8 days per week, with heavy drinking on 45.9% of the 90 days before study baseline.
Identified patients of CRAFT participants were somewhat more likely to initiate treatment.
In terms of the primary study outcome, identified patients of concerned significant others receiving internet-based CRAFT were more likely in absolute terms to initiate treatment over the 24-week study period (21.3% vs. 10.6% for waitlisted controls), however this difference just missed statistical significance, meaning we can’t with a high degree of confidence rule out the possibility this difference was due to chance and not because internet-based CRAFT produced better outcomes.
Internet-based CRAFT and the assessment-only comparison group had similar reductions in number of days of alcohol use, mean number of drinks consumed per week, and days of heavy drinking over the 24-week.
Concerned significant others showed improvements in mental health and well-being that were not sustained over time.
Concerned significant others in the internet-based CRAFT group showed a reduction in depressive symptoms and increases in quality of life and relational satisfaction with the identified patient, from baseline to 6-week follow-up, while the control group showed no meaningful change in these measures. These differences, however, were no longer apparent at 12 or 24-week follow-up.
In terms of anxiety, stress, and emotional avoidance, no meaningful between-group differences were observed at 6, 12, or 24-week follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Family members and partners of individuals with an alcohol or other drug use disorder are often severely affected by their loved one’s alcohol/drug problem but struggle greatly in effectively helping their loved one to accept treatment. Furthermore, alcohol and other drug treatments that include concerned significant others in the substance use disorder treatment process are known to produce better outcomes. As one of very few interventions for concerned significant others that empowers individuals to steer identified patients to treatment, the CRAFT intervention has tremendous potential. A recent meta-analysis of previous clinical trials found that CRAFT is approximately twice as effective as no intervention in terms of getting a loved one into substance use disorder treatment. Stylistically, it is very different from mutual-help programs and psychotherapies that encourage concerned significant others to “detach with love” (e.g., Al-Anon) and allow identified patients to ‘hit their bottom,’ or use confrontation to press a loved one to get substance use disorder treatment (e.g., Johnson interventions).
At the same time, finding a CRAFT trained provider can be challenging, which greatly reduces the public health utility of this intervention. An online version of CRAFT, in which concerned significant others can access in their own time from anywhere, is therefore an exciting proposition.
The researchers in this study, who developed and tested an online version of CRAFT, found some benefits for this version of the intervention, however, the overall pattern of results suggested internet-based CRAFT may not perform as well as in-person, provider-delivered CRAFT, which has previously been assessed and shown benefit in a number of separate clinical trials (see this paper for a recent review).
Some differences between provider-delivered CRAFT and an online version perhaps should be expected. Though essentially the same material was presented in both versions, in-person CRAFT includes more sessions (~12 vs. 5) allowing concerned significant others more time to digest the material, while also providing 10-12 weeks of professional support. Relatedly, it’s likely that some of CRAFT’s benefits come from the non-specific treatment effects that occur across therapy modalities through interacting with a provider who is validating feelings and giving vital encouragement and psychological support. More facetime with the provider is likely to provide more of these non-specific therapeutic effects.
It’s possible that internet-based versions of CRAFT would be better delivered over more than 5 sessions so the training material can be unpacked more slowly. However, given participants only completed an average of 3 of the 5 internet-based CRAFT sessions in this study, increasing the number of sessions might have a net detrimental effect by leading to more drop-out. Clinician support seems to help people stick with it longer.
Another benefit of clinician-delivered CRAFT over internet-based CRAFT is the opportunity for real-time feedback. Though internet-based CRAFT participants did get written feedback on their answers to in-session questions and homework, this feedback was not provided in real time, and doesn’t allow for a back-and-forth with the provider which would likely facilitate better, more targeted, coaching and learning.
Confidence in the findings from this study are tempered by high participant attrition (only 65% of participants completed the 24-week assessment). In such cases, it is hard to know how study dropout might have affected results. It’s possible, for instance, that participants who were doing more poorly were less likely to complete the study follow-ups, which could potentially give a distorted view of participants functioning and well-being over follow-up. This is particularly problematic when drop-out rates are unequal between study groups, as was the case in this study, with 43% of CRAFT participants not completing the 24-week assessment versus 28% of controls.
Ultimately, the differences between internet-based CRAFT and traditional clinical delivered CRAFT should be considered in light of the important issue of CRAFT’s availability. Even though internet-based CRAFT has some significant short-comings, it also has some key benefits in that it is more accessible and convenient than traditional, clinician-delivered CRAFT. Also, in this study it appeared to confer some benefits. Though between group differences in terms of number of identified patients going to treatment over the 24-week study observation period were not statistically significant, there was a meaningful doubling in the number of internet-based CRAFT participants who’s loved one entered treatment. Also, over the first 6 weeks of the study, concerned significant others had greater well-being than controls, and their identified patients drank less.
Given the enormous potential of an online version of CRAFT to reach so many family members in need, these preliminary findings suggest more work is warranted to further develop and test the internet-based CRAFT model. It’s possible community-based programs like Learn2Cope, which provide social support and information to family members of people with addiction, could complement internet-based CRAFT. These kinds of questions are very much worthy of further investigation.
As noted by the authors:
Study recruitment was slow, ultimately leading the researchers to stop recruitment before reaching their target of 140 participants. This could represent a lack of interest in CRAFT in Sweden or Western countries more broadly, or simply a lack of awareness of the intervention and its potential benefits.
Only 27 of 47 participants in the CRAFT group (57.4%) were retained in the study at 24-week follow-up, versus 34 of 47 participants in the waitlist control group (72.3%). This could be indicative of dissatisfaction with the internet-based CRAFT intervention, though is more likely a function of waitlisted controls wanting to stay engaged in the study in order to receive CRAFT training at the end of their study participation. Future studies will ideally use an ‘intent-to-treat’ design, in which participants who drop out are assumed to have had a poor treatment response.Also:
Identified patients’ treatment engagement and alcohol use was assessed via concerned significant other’s self-report, rather than direct report from the identified patient or biological verification. It’s possible some under- or over-reporting occurred.
This study focused on identified patients with alcohol use disorder. Though there’s no reason to think these findings would not generalize to identified patients with addiction to drugs other than alcohol, future studies should test this.
This investigation ended up receiving interest in the study from a sample of concerned significant others that was almost entirely Although, women may be the most affected and interested in such studies (as has been the case in US studies), future research would ideally purposely include more men and test the internet-based CRAFT model with more gender-diverse samples.
BOTTOM LINE
Previous studies suggest Community Reinforcement Approach and Family Training (CRAFT) is a helpful intervention for getting identified patients into treatment sooner, reducing their substance use, and increasing the well-being of concerned significant others. Though the internet-based version of CRAFT tested here appeared to produce some benefits, especially over the first 6 weeks of the study, most of these benefits were not sustained at 12 and 24-week follow-up. Also, confidence in these findings is undermined by high rates of study non-completion. While this internet-based version of CRAFT is promising, this study suggests that more work is needed to fine-tune and test this CRAFT version. At the same time, this work represents an initial pilot study, and can be framed as an important first step in the development and testing of an online version of CRAFT.
For individuals and families seeking recovery: Though more research is needed before an online version of CRAFT is ready to be rolled out nationally, results from this study are promising and online CRAFT training is available through such places as www.alliesinrecovery.net. If you are unable to find a trained provider in your region or through teletherapy services, this might be a helpful option. Clinician-delivered CRAFT is a well-established intervention that has been shown to get identified patients into treatment quicker, while helping to reduce their substance use, and also improve the well-being of the concerned significant others. The increasing move toward telehealth has made it easier for concerned significant others to find CRAFT trained providers. Though you may not have a CRAFT provider in your town, it’s possible there are providers in other states/territories who can provide this service.
For treatment professionals and treatment systems: CRAFT offers a different perspective to traditional “detaching with love,’ ‘tough-love,’ and confrontational approaches to managing a loved-one’s substance use disorder. Though more research is needed to establish the helpfulness of an online version of CRAFT, clinician-delivered CRAFT is a well-established intervention that has been shown to get identified patients into treatment quicker, while helping to reduce their substance use, and improve the well-being of the concerned significant others.
For scientists: An internet-based version of CRAFT that is affordable and accessible is an exciting prospect because it could greatly expand the number of people who can benefit from this intervention. These researchers’ internet-based CRAFT model has much promise, but more research is needed to fine tune and rigorously test this approach. Dismantling studies can help to determine which aspects of CRAFT are accounting for its benefit to help inform the most efficient ways to deliver this unique family-centered approach.
For policy makers: While the internet-based version of CRAFT tested in this study will require additional development and testing before being ready to scale up, traditional, provider-delivered CRAFT is known to be an effective for getting loved ones into substance use disorder treatment quicker while improving the well-being of concerned significant others. Measures that compel insurers to reimburse for CRAFT could indirectly improve public health and be economically beneficial by getting people with substance use disorder into treatment faster.
Engaging individuals in substance use disorder treatment can be incredibly challenging. Community Reinforcement Approach and Family Training (known by the acronym CRAFT) is a relatively brief intervention designed to help loved ones of people with substance use disorder get their loved one to reduce or stop their substance use, engage with treatment, while better caring for themselves. CRAFT is usually delivered over the course of 10-12 therapy sessions with a trained provider. What makes CRAFT unique is that it engages the concerned significant other/s without directly engaging the identified patient (also referred to as the concerned significant other’s “loved one”). The intervention is largely based on established principles of behavioral psychology, which can be used to shape behavior change, mostly by providing or withdrawing different types of natural rewards in the home environment (e.g., rewarding pro-recovery behaviors; withdrawing attention when substance use persists).
To increase access to CRAFT, the researchers in this study developed an internet-delivered version, which condensed clinician-delivered CRAFT into 5 brief video modules along with some online training materials. In this internet-delivered version of CRAFT, participants complete online worksheets during classes, as well as related homework assignments, which are independently reviewed by a CRAFT trained provider, who later provides written feedback through the online portal. There was no live-time (i.e., “synchronous”) communication between patients and providers.
The researchers tested their internet-delivered version of CRAFT in a controlled trial to determine whether this intervention would produce similar outcomes to previous clinical trials of traditional, clinician-delivered CRAFT.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized, waitlist-controlled trial with 94 concerned significant others with a treatment-reluctant loved one with alcohol use disorder (based on the concerned significant other’s report). Participants received 5 online sessions of CRAFT with asynchronous online support from a CRAFT trained clinician or were randomized to a waitlist-control group. All participants, recruited nationwide in Sweden, were assessed at study baseline, and then again at 6, 12, and 24-weeks after entering the study.
The internet-delivered CRAFT intervention included, 1) An overview of CRAFT’s structure designed to bolster concerned significant other’s motivation to engage with the intervention, 2) self-care strategies to help concerned significant others improve their own well-being, 3) strategies designed to maximize the likelihood the identified patient will seek treatment when asked, 4) communication skills, and 5) behavioral reinforcement skills. Click here for a more detailed description of the CRAFT intervention.
Each session included a combination of short video clips, exercises designed to help the concerned significant others learn new skills, and homework assignments to practice these skills. Participants’ responses to the session exercises and their homework assignments were reported in text to a study therapist through the researchers’ CRAFT platform. The therapist gave written feedback on their own time (i.e., asynchronously) based on the established CRAFT protocol through the internet-based CRAFT system. There was no live-time (i.e., synchronous) in-person contact between participants and study therapists. Although the active treatment period lasted 5 weeks, participants had access to web-based CRAFT for the entire 24-week study period.
Participants randomized to the waitlist control group received the same assessments as participants randomized to receive internet-based CRAFT but were only invited to receive the intervention after completing the study. For the purposes of this study, the waitlist condition was equivalent to an assessment-only comparison group.
The main study outcome was the proportion of identified patients seeking treatment for substance use disorder over the course of the 24-week follow-up period. Secondary outcomes included change in identified patients’ alcohol use from baseline to 6, 12 and 24-week follow-up, concerned significant others’ depression, anxiety, stress, and well-being, as well as their relational satisfaction with the identified patient.
Inclusion criteria for concerned significant others were: 1) Having an ongoing relationship with a treatment resistant identified patient meeting the Diagnostic and Statistical Manual of Mental Disorders IV (commonly referred to as DSM-IV) diagnosis of alcohol dependence or abuse based on diagnostic information provided by the participant (not the identified patient), 2) being at least 18 years of age, 3) spending significant time with the identified patient, defined as greater than 40% of the last 90 days, 4) confirmation from the concerned significant other that their identified patient had consumed alcohol in at least 30 of the past 90 days, and 5) having a goal of engaging the identified patient in treatment.
Exclusion criteria were: 1) Identified patients not being treatment resistant [i.e. they would seek treatment if asked], 2) identified patients receiving alcohol-related treatment within the past 6 months, 3) major psychiatric or physical illness in the concerned significant other or identified patient, 4) the identified patient having a DSM-IV diagnosis of substance dependence or abuse [not including alcohol or nicotine], 5) insufficient Swedish language comprehension, 6) participation in a concerned significant other mutual-support program like Al-Anon in the past 12 months, and 7) risk for domestic violence by the identified patient.
WHAT DID THIS STUDY FIND?
Participants were mostly female and in a partner relationship with the identified patient.
Almost all study participants identified as female (97.9%) and 86.2% were in a partner relationship with the identified patient. Concerned significant others randomized to the internet-based CRAFT group completed on average 3 of the 5 CRAFT online sessions. Per participant report, identified patients consumed an average of 5.4 drinks per day on 4.8 days per week, with heavy drinking on 45.9% of the 90 days before study baseline.
Identified patients of CRAFT participants were somewhat more likely to initiate treatment.
In terms of the primary study outcome, identified patients of concerned significant others receiving internet-based CRAFT were more likely in absolute terms to initiate treatment over the 24-week study period (21.3% vs. 10.6% for waitlisted controls), however this difference just missed statistical significance, meaning we can’t with a high degree of confidence rule out the possibility this difference was due to chance and not because internet-based CRAFT produced better outcomes.
Internet-based CRAFT and the assessment-only comparison group had similar reductions in number of days of alcohol use, mean number of drinks consumed per week, and days of heavy drinking over the 24-week.
Concerned significant others showed improvements in mental health and well-being that were not sustained over time.
Concerned significant others in the internet-based CRAFT group showed a reduction in depressive symptoms and increases in quality of life and relational satisfaction with the identified patient, from baseline to 6-week follow-up, while the control group showed no meaningful change in these measures. These differences, however, were no longer apparent at 12 or 24-week follow-up.
In terms of anxiety, stress, and emotional avoidance, no meaningful between-group differences were observed at 6, 12, or 24-week follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Family members and partners of individuals with an alcohol or other drug use disorder are often severely affected by their loved one’s alcohol/drug problem but struggle greatly in effectively helping their loved one to accept treatment. Furthermore, alcohol and other drug treatments that include concerned significant others in the substance use disorder treatment process are known to produce better outcomes. As one of very few interventions for concerned significant others that empowers individuals to steer identified patients to treatment, the CRAFT intervention has tremendous potential. A recent meta-analysis of previous clinical trials found that CRAFT is approximately twice as effective as no intervention in terms of getting a loved one into substance use disorder treatment. Stylistically, it is very different from mutual-help programs and psychotherapies that encourage concerned significant others to “detach with love” (e.g., Al-Anon) and allow identified patients to ‘hit their bottom,’ or use confrontation to press a loved one to get substance use disorder treatment (e.g., Johnson interventions).
At the same time, finding a CRAFT trained provider can be challenging, which greatly reduces the public health utility of this intervention. An online version of CRAFT, in which concerned significant others can access in their own time from anywhere, is therefore an exciting proposition.
The researchers in this study, who developed and tested an online version of CRAFT, found some benefits for this version of the intervention, however, the overall pattern of results suggested internet-based CRAFT may not perform as well as in-person, provider-delivered CRAFT, which has previously been assessed and shown benefit in a number of separate clinical trials (see this paper for a recent review).
Some differences between provider-delivered CRAFT and an online version perhaps should be expected. Though essentially the same material was presented in both versions, in-person CRAFT includes more sessions (~12 vs. 5) allowing concerned significant others more time to digest the material, while also providing 10-12 weeks of professional support. Relatedly, it’s likely that some of CRAFT’s benefits come from the non-specific treatment effects that occur across therapy modalities through interacting with a provider who is validating feelings and giving vital encouragement and psychological support. More facetime with the provider is likely to provide more of these non-specific therapeutic effects.
It’s possible that internet-based versions of CRAFT would be better delivered over more than 5 sessions so the training material can be unpacked more slowly. However, given participants only completed an average of 3 of the 5 internet-based CRAFT sessions in this study, increasing the number of sessions might have a net detrimental effect by leading to more drop-out. Clinician support seems to help people stick with it longer.
Another benefit of clinician-delivered CRAFT over internet-based CRAFT is the opportunity for real-time feedback. Though internet-based CRAFT participants did get written feedback on their answers to in-session questions and homework, this feedback was not provided in real time, and doesn’t allow for a back-and-forth with the provider which would likely facilitate better, more targeted, coaching and learning.
Confidence in the findings from this study are tempered by high participant attrition (only 65% of participants completed the 24-week assessment). In such cases, it is hard to know how study dropout might have affected results. It’s possible, for instance, that participants who were doing more poorly were less likely to complete the study follow-ups, which could potentially give a distorted view of participants functioning and well-being over follow-up. This is particularly problematic when drop-out rates are unequal between study groups, as was the case in this study, with 43% of CRAFT participants not completing the 24-week assessment versus 28% of controls.
Ultimately, the differences between internet-based CRAFT and traditional clinical delivered CRAFT should be considered in light of the important issue of CRAFT’s availability. Even though internet-based CRAFT has some significant short-comings, it also has some key benefits in that it is more accessible and convenient than traditional, clinician-delivered CRAFT. Also, in this study it appeared to confer some benefits. Though between group differences in terms of number of identified patients going to treatment over the 24-week study observation period were not statistically significant, there was a meaningful doubling in the number of internet-based CRAFT participants who’s loved one entered treatment. Also, over the first 6 weeks of the study, concerned significant others had greater well-being than controls, and their identified patients drank less.
Given the enormous potential of an online version of CRAFT to reach so many family members in need, these preliminary findings suggest more work is warranted to further develop and test the internet-based CRAFT model. It’s possible community-based programs like Learn2Cope, which provide social support and information to family members of people with addiction, could complement internet-based CRAFT. These kinds of questions are very much worthy of further investigation.
As noted by the authors:
Study recruitment was slow, ultimately leading the researchers to stop recruitment before reaching their target of 140 participants. This could represent a lack of interest in CRAFT in Sweden or Western countries more broadly, or simply a lack of awareness of the intervention and its potential benefits.
Only 27 of 47 participants in the CRAFT group (57.4%) were retained in the study at 24-week follow-up, versus 34 of 47 participants in the waitlist control group (72.3%). This could be indicative of dissatisfaction with the internet-based CRAFT intervention, though is more likely a function of waitlisted controls wanting to stay engaged in the study in order to receive CRAFT training at the end of their study participation. Future studies will ideally use an ‘intent-to-treat’ design, in which participants who drop out are assumed to have had a poor treatment response.Also:
Identified patients’ treatment engagement and alcohol use was assessed via concerned significant other’s self-report, rather than direct report from the identified patient or biological verification. It’s possible some under- or over-reporting occurred.
This study focused on identified patients with alcohol use disorder. Though there’s no reason to think these findings would not generalize to identified patients with addiction to drugs other than alcohol, future studies should test this.
This investigation ended up receiving interest in the study from a sample of concerned significant others that was almost entirely Although, women may be the most affected and interested in such studies (as has been the case in US studies), future research would ideally purposely include more men and test the internet-based CRAFT model with more gender-diverse samples.
BOTTOM LINE
Previous studies suggest Community Reinforcement Approach and Family Training (CRAFT) is a helpful intervention for getting identified patients into treatment sooner, reducing their substance use, and increasing the well-being of concerned significant others. Though the internet-based version of CRAFT tested here appeared to produce some benefits, especially over the first 6 weeks of the study, most of these benefits were not sustained at 12 and 24-week follow-up. Also, confidence in these findings is undermined by high rates of study non-completion. While this internet-based version of CRAFT is promising, this study suggests that more work is needed to fine-tune and test this CRAFT version. At the same time, this work represents an initial pilot study, and can be framed as an important first step in the development and testing of an online version of CRAFT.
For individuals and families seeking recovery: Though more research is needed before an online version of CRAFT is ready to be rolled out nationally, results from this study are promising and online CRAFT training is available through such places as www.alliesinrecovery.net. If you are unable to find a trained provider in your region or through teletherapy services, this might be a helpful option. Clinician-delivered CRAFT is a well-established intervention that has been shown to get identified patients into treatment quicker, while helping to reduce their substance use, and also improve the well-being of the concerned significant others. The increasing move toward telehealth has made it easier for concerned significant others to find CRAFT trained providers. Though you may not have a CRAFT provider in your town, it’s possible there are providers in other states/territories who can provide this service.
For treatment professionals and treatment systems: CRAFT offers a different perspective to traditional “detaching with love,’ ‘tough-love,’ and confrontational approaches to managing a loved-one’s substance use disorder. Though more research is needed to establish the helpfulness of an online version of CRAFT, clinician-delivered CRAFT is a well-established intervention that has been shown to get identified patients into treatment quicker, while helping to reduce their substance use, and improve the well-being of the concerned significant others.
For scientists: An internet-based version of CRAFT that is affordable and accessible is an exciting prospect because it could greatly expand the number of people who can benefit from this intervention. These researchers’ internet-based CRAFT model has much promise, but more research is needed to fine tune and rigorously test this approach. Dismantling studies can help to determine which aspects of CRAFT are accounting for its benefit to help inform the most efficient ways to deliver this unique family-centered approach.
For policy makers: While the internet-based version of CRAFT tested in this study will require additional development and testing before being ready to scale up, traditional, provider-delivered CRAFT is known to be an effective for getting loved ones into substance use disorder treatment quicker while improving the well-being of concerned significant others. Measures that compel insurers to reimburse for CRAFT could indirectly improve public health and be economically beneficial by getting people with substance use disorder into treatment faster.
Engaging individuals in substance use disorder treatment can be incredibly challenging. Community Reinforcement Approach and Family Training (known by the acronym CRAFT) is a relatively brief intervention designed to help loved ones of people with substance use disorder get their loved one to reduce or stop their substance use, engage with treatment, while better caring for themselves. CRAFT is usually delivered over the course of 10-12 therapy sessions with a trained provider. What makes CRAFT unique is that it engages the concerned significant other/s without directly engaging the identified patient (also referred to as the concerned significant other’s “loved one”). The intervention is largely based on established principles of behavioral psychology, which can be used to shape behavior change, mostly by providing or withdrawing different types of natural rewards in the home environment (e.g., rewarding pro-recovery behaviors; withdrawing attention when substance use persists).
To increase access to CRAFT, the researchers in this study developed an internet-delivered version, which condensed clinician-delivered CRAFT into 5 brief video modules along with some online training materials. In this internet-delivered version of CRAFT, participants complete online worksheets during classes, as well as related homework assignments, which are independently reviewed by a CRAFT trained provider, who later provides written feedback through the online portal. There was no live-time (i.e., “synchronous”) communication between patients and providers.
The researchers tested their internet-delivered version of CRAFT in a controlled trial to determine whether this intervention would produce similar outcomes to previous clinical trials of traditional, clinician-delivered CRAFT.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized, waitlist-controlled trial with 94 concerned significant others with a treatment-reluctant loved one with alcohol use disorder (based on the concerned significant other’s report). Participants received 5 online sessions of CRAFT with asynchronous online support from a CRAFT trained clinician or were randomized to a waitlist-control group. All participants, recruited nationwide in Sweden, were assessed at study baseline, and then again at 6, 12, and 24-weeks after entering the study.
The internet-delivered CRAFT intervention included, 1) An overview of CRAFT’s structure designed to bolster concerned significant other’s motivation to engage with the intervention, 2) self-care strategies to help concerned significant others improve their own well-being, 3) strategies designed to maximize the likelihood the identified patient will seek treatment when asked, 4) communication skills, and 5) behavioral reinforcement skills. Click here for a more detailed description of the CRAFT intervention.
Each session included a combination of short video clips, exercises designed to help the concerned significant others learn new skills, and homework assignments to practice these skills. Participants’ responses to the session exercises and their homework assignments were reported in text to a study therapist through the researchers’ CRAFT platform. The therapist gave written feedback on their own time (i.e., asynchronously) based on the established CRAFT protocol through the internet-based CRAFT system. There was no live-time (i.e., synchronous) in-person contact between participants and study therapists. Although the active treatment period lasted 5 weeks, participants had access to web-based CRAFT for the entire 24-week study period.
Participants randomized to the waitlist control group received the same assessments as participants randomized to receive internet-based CRAFT but were only invited to receive the intervention after completing the study. For the purposes of this study, the waitlist condition was equivalent to an assessment-only comparison group.
The main study outcome was the proportion of identified patients seeking treatment for substance use disorder over the course of the 24-week follow-up period. Secondary outcomes included change in identified patients’ alcohol use from baseline to 6, 12 and 24-week follow-up, concerned significant others’ depression, anxiety, stress, and well-being, as well as their relational satisfaction with the identified patient.
Inclusion criteria for concerned significant others were: 1) Having an ongoing relationship with a treatment resistant identified patient meeting the Diagnostic and Statistical Manual of Mental Disorders IV (commonly referred to as DSM-IV) diagnosis of alcohol dependence or abuse based on diagnostic information provided by the participant (not the identified patient), 2) being at least 18 years of age, 3) spending significant time with the identified patient, defined as greater than 40% of the last 90 days, 4) confirmation from the concerned significant other that their identified patient had consumed alcohol in at least 30 of the past 90 days, and 5) having a goal of engaging the identified patient in treatment.
Exclusion criteria were: 1) Identified patients not being treatment resistant [i.e. they would seek treatment if asked], 2) identified patients receiving alcohol-related treatment within the past 6 months, 3) major psychiatric or physical illness in the concerned significant other or identified patient, 4) the identified patient having a DSM-IV diagnosis of substance dependence or abuse [not including alcohol or nicotine], 5) insufficient Swedish language comprehension, 6) participation in a concerned significant other mutual-support program like Al-Anon in the past 12 months, and 7) risk for domestic violence by the identified patient.
WHAT DID THIS STUDY FIND?
Participants were mostly female and in a partner relationship with the identified patient.
Almost all study participants identified as female (97.9%) and 86.2% were in a partner relationship with the identified patient. Concerned significant others randomized to the internet-based CRAFT group completed on average 3 of the 5 CRAFT online sessions. Per participant report, identified patients consumed an average of 5.4 drinks per day on 4.8 days per week, with heavy drinking on 45.9% of the 90 days before study baseline.
Identified patients of CRAFT participants were somewhat more likely to initiate treatment.
In terms of the primary study outcome, identified patients of concerned significant others receiving internet-based CRAFT were more likely in absolute terms to initiate treatment over the 24-week study period (21.3% vs. 10.6% for waitlisted controls), however this difference just missed statistical significance, meaning we can’t with a high degree of confidence rule out the possibility this difference was due to chance and not because internet-based CRAFT produced better outcomes.
Internet-based CRAFT and the assessment-only comparison group had similar reductions in number of days of alcohol use, mean number of drinks consumed per week, and days of heavy drinking over the 24-week.
Concerned significant others showed improvements in mental health and well-being that were not sustained over time.
Concerned significant others in the internet-based CRAFT group showed a reduction in depressive symptoms and increases in quality of life and relational satisfaction with the identified patient, from baseline to 6-week follow-up, while the control group showed no meaningful change in these measures. These differences, however, were no longer apparent at 12 or 24-week follow-up.
In terms of anxiety, stress, and emotional avoidance, no meaningful between-group differences were observed at 6, 12, or 24-week follow-up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Family members and partners of individuals with an alcohol or other drug use disorder are often severely affected by their loved one’s alcohol/drug problem but struggle greatly in effectively helping their loved one to accept treatment. Furthermore, alcohol and other drug treatments that include concerned significant others in the substance use disorder treatment process are known to produce better outcomes. As one of very few interventions for concerned significant others that empowers individuals to steer identified patients to treatment, the CRAFT intervention has tremendous potential. A recent meta-analysis of previous clinical trials found that CRAFT is approximately twice as effective as no intervention in terms of getting a loved one into substance use disorder treatment. Stylistically, it is very different from mutual-help programs and psychotherapies that encourage concerned significant others to “detach with love” (e.g., Al-Anon) and allow identified patients to ‘hit their bottom,’ or use confrontation to press a loved one to get substance use disorder treatment (e.g., Johnson interventions).
At the same time, finding a CRAFT trained provider can be challenging, which greatly reduces the public health utility of this intervention. An online version of CRAFT, in which concerned significant others can access in their own time from anywhere, is therefore an exciting proposition.
The researchers in this study, who developed and tested an online version of CRAFT, found some benefits for this version of the intervention, however, the overall pattern of results suggested internet-based CRAFT may not perform as well as in-person, provider-delivered CRAFT, which has previously been assessed and shown benefit in a number of separate clinical trials (see this paper for a recent review).
Some differences between provider-delivered CRAFT and an online version perhaps should be expected. Though essentially the same material was presented in both versions, in-person CRAFT includes more sessions (~12 vs. 5) allowing concerned significant others more time to digest the material, while also providing 10-12 weeks of professional support. Relatedly, it’s likely that some of CRAFT’s benefits come from the non-specific treatment effects that occur across therapy modalities through interacting with a provider who is validating feelings and giving vital encouragement and psychological support. More facetime with the provider is likely to provide more of these non-specific therapeutic effects.
It’s possible that internet-based versions of CRAFT would be better delivered over more than 5 sessions so the training material can be unpacked more slowly. However, given participants only completed an average of 3 of the 5 internet-based CRAFT sessions in this study, increasing the number of sessions might have a net detrimental effect by leading to more drop-out. Clinician support seems to help people stick with it longer.
Another benefit of clinician-delivered CRAFT over internet-based CRAFT is the opportunity for real-time feedback. Though internet-based CRAFT participants did get written feedback on their answers to in-session questions and homework, this feedback was not provided in real time, and doesn’t allow for a back-and-forth with the provider which would likely facilitate better, more targeted, coaching and learning.
Confidence in the findings from this study are tempered by high participant attrition (only 65% of participants completed the 24-week assessment). In such cases, it is hard to know how study dropout might have affected results. It’s possible, for instance, that participants who were doing more poorly were less likely to complete the study follow-ups, which could potentially give a distorted view of participants functioning and well-being over follow-up. This is particularly problematic when drop-out rates are unequal between study groups, as was the case in this study, with 43% of CRAFT participants not completing the 24-week assessment versus 28% of controls.
Ultimately, the differences between internet-based CRAFT and traditional clinical delivered CRAFT should be considered in light of the important issue of CRAFT’s availability. Even though internet-based CRAFT has some significant short-comings, it also has some key benefits in that it is more accessible and convenient than traditional, clinician-delivered CRAFT. Also, in this study it appeared to confer some benefits. Though between group differences in terms of number of identified patients going to treatment over the 24-week study observation period were not statistically significant, there was a meaningful doubling in the number of internet-based CRAFT participants who’s loved one entered treatment. Also, over the first 6 weeks of the study, concerned significant others had greater well-being than controls, and their identified patients drank less.
Given the enormous potential of an online version of CRAFT to reach so many family members in need, these preliminary findings suggest more work is warranted to further develop and test the internet-based CRAFT model. It’s possible community-based programs like Learn2Cope, which provide social support and information to family members of people with addiction, could complement internet-based CRAFT. These kinds of questions are very much worthy of further investigation.
As noted by the authors:
Study recruitment was slow, ultimately leading the researchers to stop recruitment before reaching their target of 140 participants. This could represent a lack of interest in CRAFT in Sweden or Western countries more broadly, or simply a lack of awareness of the intervention and its potential benefits.
Only 27 of 47 participants in the CRAFT group (57.4%) were retained in the study at 24-week follow-up, versus 34 of 47 participants in the waitlist control group (72.3%). This could be indicative of dissatisfaction with the internet-based CRAFT intervention, though is more likely a function of waitlisted controls wanting to stay engaged in the study in order to receive CRAFT training at the end of their study participation. Future studies will ideally use an ‘intent-to-treat’ design, in which participants who drop out are assumed to have had a poor treatment response.Also:
Identified patients’ treatment engagement and alcohol use was assessed via concerned significant other’s self-report, rather than direct report from the identified patient or biological verification. It’s possible some under- or over-reporting occurred.
This study focused on identified patients with alcohol use disorder. Though there’s no reason to think these findings would not generalize to identified patients with addiction to drugs other than alcohol, future studies should test this.
This investigation ended up receiving interest in the study from a sample of concerned significant others that was almost entirely Although, women may be the most affected and interested in such studies (as has been the case in US studies), future research would ideally purposely include more men and test the internet-based CRAFT model with more gender-diverse samples.
BOTTOM LINE
Previous studies suggest Community Reinforcement Approach and Family Training (CRAFT) is a helpful intervention for getting identified patients into treatment sooner, reducing their substance use, and increasing the well-being of concerned significant others. Though the internet-based version of CRAFT tested here appeared to produce some benefits, especially over the first 6 weeks of the study, most of these benefits were not sustained at 12 and 24-week follow-up. Also, confidence in these findings is undermined by high rates of study non-completion. While this internet-based version of CRAFT is promising, this study suggests that more work is needed to fine-tune and test this CRAFT version. At the same time, this work represents an initial pilot study, and can be framed as an important first step in the development and testing of an online version of CRAFT.
For individuals and families seeking recovery: Though more research is needed before an online version of CRAFT is ready to be rolled out nationally, results from this study are promising and online CRAFT training is available through such places as www.alliesinrecovery.net. If you are unable to find a trained provider in your region or through teletherapy services, this might be a helpful option. Clinician-delivered CRAFT is a well-established intervention that has been shown to get identified patients into treatment quicker, while helping to reduce their substance use, and also improve the well-being of the concerned significant others. The increasing move toward telehealth has made it easier for concerned significant others to find CRAFT trained providers. Though you may not have a CRAFT provider in your town, it’s possible there are providers in other states/territories who can provide this service.
For treatment professionals and treatment systems: CRAFT offers a different perspective to traditional “detaching with love,’ ‘tough-love,’ and confrontational approaches to managing a loved-one’s substance use disorder. Though more research is needed to establish the helpfulness of an online version of CRAFT, clinician-delivered CRAFT is a well-established intervention that has been shown to get identified patients into treatment quicker, while helping to reduce their substance use, and improve the well-being of the concerned significant others.
For scientists: An internet-based version of CRAFT that is affordable and accessible is an exciting prospect because it could greatly expand the number of people who can benefit from this intervention. These researchers’ internet-based CRAFT model has much promise, but more research is needed to fine tune and rigorously test this approach. Dismantling studies can help to determine which aspects of CRAFT are accounting for its benefit to help inform the most efficient ways to deliver this unique family-centered approach.
For policy makers: While the internet-based version of CRAFT tested in this study will require additional development and testing before being ready to scale up, traditional, provider-delivered CRAFT is known to be an effective for getting loved ones into substance use disorder treatment quicker while improving the well-being of concerned significant others. Measures that compel insurers to reimburse for CRAFT could indirectly improve public health and be economically beneficial by getting people with substance use disorder into treatment faster.