Cannabis use during adolescence is linked to a range of mental and physical health consequences. This study investigated if cannabis use disorder was associated with suicide and self-harm behaviors in adolescents.

Adolescence is a unique developmental stage that can be complicated and disrupted by alcohol and other drug use (i.e., substance use). During adolescence, substance use increases risk for disruptions to brain structures and functions implicated in reward as well as impaired memory and reduced cognitive performance. Understanding the correlates and consequences of adolescent substance use may both help address and prevent the harms of substance use while also reducing the time it takes to initiate problem resolution and recovery.
Suicide is the third leading cause of death in US adolescents. Substance use broadly has been linked with suicide and related behaviors. However, there has been little work to understand how individual substances or substance use disorders are associated with suicide and self-harm among young people. Cannabis use specifically, may be linked with developmental consequences that increase risk for impulsive decision making, depression, and anxiety, all of which are directly related to increased risk of suicidal behaviors. Furthermore, after alcohol, cannabis is the most commonly used substance among adolescents, which may continue to change due to shifting cannabis policies and corresponding social norm changes. For example, the legalization of recreational cannabis sales has led to decreased perceptions of cannabis use related harm among adolescents in many states. One theory suggests cannabis use during this important stage of neurodevelopment may impair emotion regulation, thereby increasing impulsivity and the likelihood of maladaptive behaviors, including but not limited to suicidal behaviors. Understanding how cannabis use and cannabis use disorder may be directly and indirectly linked with suicide and self-harm may inform clinical practices (i.e., screening during primary care) for adolescents and inform treatment and recovery planning.
This study used a large, nationwide database of inpatient health records to explore the relationship between cannabis use disorder and suicide/self-harm as well as how depression may change that relationship. The Nationwide Inpatient Sample (NIS) database is administered by the Agency for Healthcare Research and Quality as part of the Healthcare Cost and Utilization Project. It is a publicly available, all-payer inpatient care database designed to produce regional and national estimates of inpatient use, access, cost, quality, and outcomes for all health services including but not limited to mental health care. For this study, all adolescent (aged 10-19) inpatient admissions from January 1st, 2016, through December 31st, 2019, were included—totaling 807,105 inpatient admission records.
The main variables of interest were cannabis use disorder and suicide/self-harm, which were identified using ICD-10 codes, which are international classification codes often used in research and medical billing. The study also included the co-occurrence of other disorders including, Depression, Anxiety, Eating Disorder, Attention Deficit Hyperactivity Disorder, Intellectual and Developmental Disability, Conduct Disorder, and Substance Use Disorders (Alcohol, Nicotine, Cocaine, Stimulant). All substance use and mental health diagnoses were made by clinicians; whether clinicians used a structured and validated clinical interview to determine diagnosis is not reported. Age, sex, race and primary insurance payer (i.e., public, private, self-pay) were also included in analysis. A severity of illness score known as the All Patients Refined Diagnosis Related Group score was also included, which categorized severity into four levels (minor, moderate, major, extreme) based on a primary diagnosis, secondary diagnosis, age, procedures performed during the inpatient stay, and hospital discharge status.
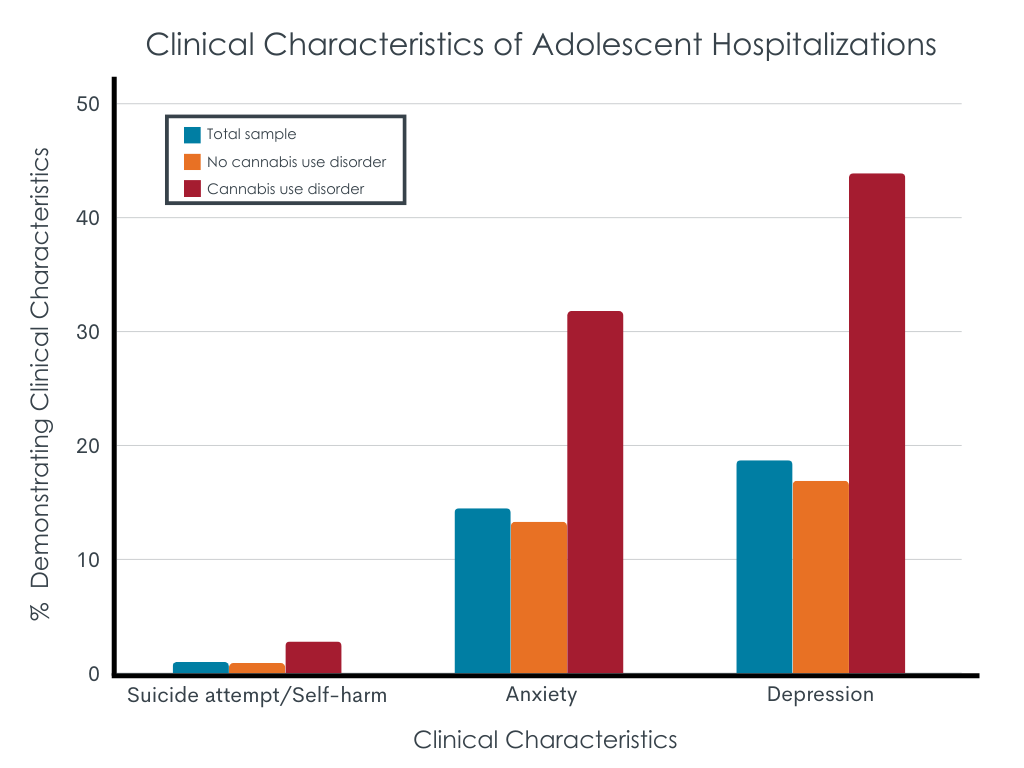
In total, 807,105 adolescents were included in the study, with 53,751 having cannabis use disorder. The average age of participants was 16 and the majority were female (62%) and White (51%). About half (55%) had public insurance, while 41% has private insurance and 4% were self-pay. The illness severity of participants was mostly minor (41%) and moderate (42%) severity, while some had major (14%) and extreme (4%) illness severity. Depression was also present among 19% of participants. Among the participants, 1% had a suicide attempt or self-harm. Similarly, 1% of those without cannabis use disorder had a suicide attempt or self-harm, but 3% of those with cannabis use orders had attempted suicide or self-harmed. Most (92%) of participants were discharged home following their inpatient stay.
Cannabis use disorder associated with increased risk for suicide attempt or self-harm.
After controlling for age, sex, race, insurance type, illness severity, and other co-occurring disorders such as depression, adolescents with cannabis use disorder had 40% greater odds of attempting suicide or self-harm compared to those without a cannabis use disorder. Of note, this increased risk was similar when examining suicide and self-harm separately.
Depression and cannabis use disorder confer unique risks.
Given the strong link between depression and suicide/self-harm found in this study, additional analysis was done to assess how depression altered the relationship between cannabis use disorder and suicide/self-harm. Adolescents with both cannabis use disorder and depression had 9 times greater odds of suicide attempt or self-harm compared to those without either cannabis use disorder or depression. For those with cannabis use disorder, the presence of depression was associated with 2 times greater odds of suicide attempt or self-harm compared to those with cannabis use disorder but no depression. For those with depression, the presence of cannabis use disorder increased the magnitude of risk for suicide attempt and self-harm – a 9-fold increased odds of suicide for those with cannabis use disorder vs. an 8.5-fold increased odds of suicide for those without cannabis use disorder, though these groups were not directly compared.
This study examined the association between cannabis use disorder and suicide/self-harm in a large, nationally representative sample of hospitalized adolescents. The study found that adolescents with cannabis use disorder were 40% more likely to experience a suicide attempt or self-harm, independent of demographic and clinical factors also associated with suicide such as depression. The observed link between cannabis use disorder and suicidal behavior suggests that screening for self-injurious behaviors among those with cannabis use disorder could be an important way to reduce harm among adolescents appearing in inpatient settings. However, the study cannot determine the direction of effect – cannabis use impacts on mental and physical health results in greater risk for suicide, cannabis use as a means to cope with increased suicidal ideation, or some reciprocal effect.
Given the relationship between cannabis use and psychotic symptoms – where cannabis exposure enhances risk for psychosis in those with pre-existing genetic vulnerabilities – it could also be that cannabis use enhances risk for suicide only if certain pre-existing risk factors are present. Notably, however, the explanation cannot be simply that depressed adolescents are both more likely to have suicidal behaviors and to use cannabis, given that analyses controlled for the presence of a set of co-occurring mental health and substance use disorders including, but not limited to, depression. Future research should explore the co-occurrence of cannabis use disorder and suicidal behaviors, the extent to which cannabis use may be causally related to suicidal behavior, and the possible mechanisms underlying this linkage. This study indicates there is a strong association between cannabis use disorder and suicidal behaviors, which should be screened and addressed across clinical settings.
This study found that adolescents who were treated in an inpatient setting and had cannabis use disorder were much more likely to engage in suicidal behaviors. Furthermore, those with depression and cannabis use disorder were at an even higher risk of attempting suicide or self-harming than those with one or the other separately. Adolescence is an important stage of development during which key neurocognitive, social, and psychological changes occur. Suicide is a leading cause of death among this age group and cannabis is being perceived as less risky among youth in part due to cannabis legalization in many states. The study was cross-sectional and cannot determine if cannabis use and cannabis use disorder led to or caused suicidal behavior. It may be that suicidal behaviors and their underlying mechanisms were making cannabis use more likely. While future research may further examine whether cannabis use and suicidal behaviors are causally related, given their co-occurrence, screenings for suicide in adolescents may be improved by assessing for cannabis and screenings for cannabis use disorder in adolescents may be improved by assessing for suicide and self-harm.
Oladunjoye, A. F., Li, E., Aneni, K., & Onigu-Otite, E. (2023). Cannabis use disorder, suicide attempts, and self-harm among adolescents: A national inpatient study across the United States. PLOS ONE, 18(10), e0292922. doi: 10.1371/journal.pone.0292922
Adolescence is a unique developmental stage that can be complicated and disrupted by alcohol and other drug use (i.e., substance use). During adolescence, substance use increases risk for disruptions to brain structures and functions implicated in reward as well as impaired memory and reduced cognitive performance. Understanding the correlates and consequences of adolescent substance use may both help address and prevent the harms of substance use while also reducing the time it takes to initiate problem resolution and recovery.
Suicide is the third leading cause of death in US adolescents. Substance use broadly has been linked with suicide and related behaviors. However, there has been little work to understand how individual substances or substance use disorders are associated with suicide and self-harm among young people. Cannabis use specifically, may be linked with developmental consequences that increase risk for impulsive decision making, depression, and anxiety, all of which are directly related to increased risk of suicidal behaviors. Furthermore, after alcohol, cannabis is the most commonly used substance among adolescents, which may continue to change due to shifting cannabis policies and corresponding social norm changes. For example, the legalization of recreational cannabis sales has led to decreased perceptions of cannabis use related harm among adolescents in many states. One theory suggests cannabis use during this important stage of neurodevelopment may impair emotion regulation, thereby increasing impulsivity and the likelihood of maladaptive behaviors, including but not limited to suicidal behaviors. Understanding how cannabis use and cannabis use disorder may be directly and indirectly linked with suicide and self-harm may inform clinical practices (i.e., screening during primary care) for adolescents and inform treatment and recovery planning.
This study used a large, nationwide database of inpatient health records to explore the relationship between cannabis use disorder and suicide/self-harm as well as how depression may change that relationship. The Nationwide Inpatient Sample (NIS) database is administered by the Agency for Healthcare Research and Quality as part of the Healthcare Cost and Utilization Project. It is a publicly available, all-payer inpatient care database designed to produce regional and national estimates of inpatient use, access, cost, quality, and outcomes for all health services including but not limited to mental health care. For this study, all adolescent (aged 10-19) inpatient admissions from January 1st, 2016, through December 31st, 2019, were included—totaling 807,105 inpatient admission records.
The main variables of interest were cannabis use disorder and suicide/self-harm, which were identified using ICD-10 codes, which are international classification codes often used in research and medical billing. The study also included the co-occurrence of other disorders including, Depression, Anxiety, Eating Disorder, Attention Deficit Hyperactivity Disorder, Intellectual and Developmental Disability, Conduct Disorder, and Substance Use Disorders (Alcohol, Nicotine, Cocaine, Stimulant). All substance use and mental health diagnoses were made by clinicians; whether clinicians used a structured and validated clinical interview to determine diagnosis is not reported. Age, sex, race and primary insurance payer (i.e., public, private, self-pay) were also included in analysis. A severity of illness score known as the All Patients Refined Diagnosis Related Group score was also included, which categorized severity into four levels (minor, moderate, major, extreme) based on a primary diagnosis, secondary diagnosis, age, procedures performed during the inpatient stay, and hospital discharge status.
In total, 807,105 adolescents were included in the study, with 53,751 having cannabis use disorder. The average age of participants was 16 and the majority were female (62%) and White (51%). About half (55%) had public insurance, while 41% has private insurance and 4% were self-pay. The illness severity of participants was mostly minor (41%) and moderate (42%) severity, while some had major (14%) and extreme (4%) illness severity. Depression was also present among 19% of participants. Among the participants, 1% had a suicide attempt or self-harm. Similarly, 1% of those without cannabis use disorder had a suicide attempt or self-harm, but 3% of those with cannabis use orders had attempted suicide or self-harmed. Most (92%) of participants were discharged home following their inpatient stay.
Cannabis use disorder associated with increased risk for suicide attempt or self-harm.
After controlling for age, sex, race, insurance type, illness severity, and other co-occurring disorders such as depression, adolescents with cannabis use disorder had 40% greater odds of attempting suicide or self-harm compared to those without a cannabis use disorder. Of note, this increased risk was similar when examining suicide and self-harm separately.
Depression and cannabis use disorder confer unique risks.
Given the strong link between depression and suicide/self-harm found in this study, additional analysis was done to assess how depression altered the relationship between cannabis use disorder and suicide/self-harm. Adolescents with both cannabis use disorder and depression had 9 times greater odds of suicide attempt or self-harm compared to those without either cannabis use disorder or depression. For those with cannabis use disorder, the presence of depression was associated with 2 times greater odds of suicide attempt or self-harm compared to those with cannabis use disorder but no depression. For those with depression, the presence of cannabis use disorder increased the magnitude of risk for suicide attempt and self-harm – a 9-fold increased odds of suicide for those with cannabis use disorder vs. an 8.5-fold increased odds of suicide for those without cannabis use disorder, though these groups were not directly compared.
This study examined the association between cannabis use disorder and suicide/self-harm in a large, nationally representative sample of hospitalized adolescents. The study found that adolescents with cannabis use disorder were 40% more likely to experience a suicide attempt or self-harm, independent of demographic and clinical factors also associated with suicide such as depression. The observed link between cannabis use disorder and suicidal behavior suggests that screening for self-injurious behaviors among those with cannabis use disorder could be an important way to reduce harm among adolescents appearing in inpatient settings. However, the study cannot determine the direction of effect – cannabis use impacts on mental and physical health results in greater risk for suicide, cannabis use as a means to cope with increased suicidal ideation, or some reciprocal effect.
Given the relationship between cannabis use and psychotic symptoms – where cannabis exposure enhances risk for psychosis in those with pre-existing genetic vulnerabilities – it could also be that cannabis use enhances risk for suicide only if certain pre-existing risk factors are present. Notably, however, the explanation cannot be simply that depressed adolescents are both more likely to have suicidal behaviors and to use cannabis, given that analyses controlled for the presence of a set of co-occurring mental health and substance use disorders including, but not limited to, depression. Future research should explore the co-occurrence of cannabis use disorder and suicidal behaviors, the extent to which cannabis use may be causally related to suicidal behavior, and the possible mechanisms underlying this linkage. This study indicates there is a strong association between cannabis use disorder and suicidal behaviors, which should be screened and addressed across clinical settings.
This study found that adolescents who were treated in an inpatient setting and had cannabis use disorder were much more likely to engage in suicidal behaviors. Furthermore, those with depression and cannabis use disorder were at an even higher risk of attempting suicide or self-harming than those with one or the other separately. Adolescence is an important stage of development during which key neurocognitive, social, and psychological changes occur. Suicide is a leading cause of death among this age group and cannabis is being perceived as less risky among youth in part due to cannabis legalization in many states. The study was cross-sectional and cannot determine if cannabis use and cannabis use disorder led to or caused suicidal behavior. It may be that suicidal behaviors and their underlying mechanisms were making cannabis use more likely. While future research may further examine whether cannabis use and suicidal behaviors are causally related, given their co-occurrence, screenings for suicide in adolescents may be improved by assessing for cannabis and screenings for cannabis use disorder in adolescents may be improved by assessing for suicide and self-harm.
Oladunjoye, A. F., Li, E., Aneni, K., & Onigu-Otite, E. (2023). Cannabis use disorder, suicide attempts, and self-harm among adolescents: A national inpatient study across the United States. PLOS ONE, 18(10), e0292922. doi: 10.1371/journal.pone.0292922






Adolescence is a unique developmental stage that can be complicated and disrupted by alcohol and other drug use (i.e., substance use). During adolescence, substance use increases risk for disruptions to brain structures and functions implicated in reward as well as impaired memory and reduced cognitive performance. Understanding the correlates and consequences of adolescent substance use may both help address and prevent the harms of substance use while also reducing the time it takes to initiate problem resolution and recovery.
Suicide is the third leading cause of death in US adolescents. Substance use broadly has been linked with suicide and related behaviors. However, there has been little work to understand how individual substances or substance use disorders are associated with suicide and self-harm among young people. Cannabis use specifically, may be linked with developmental consequences that increase risk for impulsive decision making, depression, and anxiety, all of which are directly related to increased risk of suicidal behaviors. Furthermore, after alcohol, cannabis is the most commonly used substance among adolescents, which may continue to change due to shifting cannabis policies and corresponding social norm changes. For example, the legalization of recreational cannabis sales has led to decreased perceptions of cannabis use related harm among adolescents in many states. One theory suggests cannabis use during this important stage of neurodevelopment may impair emotion regulation, thereby increasing impulsivity and the likelihood of maladaptive behaviors, including but not limited to suicidal behaviors. Understanding how cannabis use and cannabis use disorder may be directly and indirectly linked with suicide and self-harm may inform clinical practices (i.e., screening during primary care) for adolescents and inform treatment and recovery planning.
This study used a large, nationwide database of inpatient health records to explore the relationship between cannabis use disorder and suicide/self-harm as well as how depression may change that relationship. The Nationwide Inpatient Sample (NIS) database is administered by the Agency for Healthcare Research and Quality as part of the Healthcare Cost and Utilization Project. It is a publicly available, all-payer inpatient care database designed to produce regional and national estimates of inpatient use, access, cost, quality, and outcomes for all health services including but not limited to mental health care. For this study, all adolescent (aged 10-19) inpatient admissions from January 1st, 2016, through December 31st, 2019, were included—totaling 807,105 inpatient admission records.
The main variables of interest were cannabis use disorder and suicide/self-harm, which were identified using ICD-10 codes, which are international classification codes often used in research and medical billing. The study also included the co-occurrence of other disorders including, Depression, Anxiety, Eating Disorder, Attention Deficit Hyperactivity Disorder, Intellectual and Developmental Disability, Conduct Disorder, and Substance Use Disorders (Alcohol, Nicotine, Cocaine, Stimulant). All substance use and mental health diagnoses were made by clinicians; whether clinicians used a structured and validated clinical interview to determine diagnosis is not reported. Age, sex, race and primary insurance payer (i.e., public, private, self-pay) were also included in analysis. A severity of illness score known as the All Patients Refined Diagnosis Related Group score was also included, which categorized severity into four levels (minor, moderate, major, extreme) based on a primary diagnosis, secondary diagnosis, age, procedures performed during the inpatient stay, and hospital discharge status.
In total, 807,105 adolescents were included in the study, with 53,751 having cannabis use disorder. The average age of participants was 16 and the majority were female (62%) and White (51%). About half (55%) had public insurance, while 41% has private insurance and 4% were self-pay. The illness severity of participants was mostly minor (41%) and moderate (42%) severity, while some had major (14%) and extreme (4%) illness severity. Depression was also present among 19% of participants. Among the participants, 1% had a suicide attempt or self-harm. Similarly, 1% of those without cannabis use disorder had a suicide attempt or self-harm, but 3% of those with cannabis use orders had attempted suicide or self-harmed. Most (92%) of participants were discharged home following their inpatient stay.
Cannabis use disorder associated with increased risk for suicide attempt or self-harm.
After controlling for age, sex, race, insurance type, illness severity, and other co-occurring disorders such as depression, adolescents with cannabis use disorder had 40% greater odds of attempting suicide or self-harm compared to those without a cannabis use disorder. Of note, this increased risk was similar when examining suicide and self-harm separately.
Depression and cannabis use disorder confer unique risks.
Given the strong link between depression and suicide/self-harm found in this study, additional analysis was done to assess how depression altered the relationship between cannabis use disorder and suicide/self-harm. Adolescents with both cannabis use disorder and depression had 9 times greater odds of suicide attempt or self-harm compared to those without either cannabis use disorder or depression. For those with cannabis use disorder, the presence of depression was associated with 2 times greater odds of suicide attempt or self-harm compared to those with cannabis use disorder but no depression. For those with depression, the presence of cannabis use disorder increased the magnitude of risk for suicide attempt and self-harm – a 9-fold increased odds of suicide for those with cannabis use disorder vs. an 8.5-fold increased odds of suicide for those without cannabis use disorder, though these groups were not directly compared.
This study examined the association between cannabis use disorder and suicide/self-harm in a large, nationally representative sample of hospitalized adolescents. The study found that adolescents with cannabis use disorder were 40% more likely to experience a suicide attempt or self-harm, independent of demographic and clinical factors also associated with suicide such as depression. The observed link between cannabis use disorder and suicidal behavior suggests that screening for self-injurious behaviors among those with cannabis use disorder could be an important way to reduce harm among adolescents appearing in inpatient settings. However, the study cannot determine the direction of effect – cannabis use impacts on mental and physical health results in greater risk for suicide, cannabis use as a means to cope with increased suicidal ideation, or some reciprocal effect.
Given the relationship between cannabis use and psychotic symptoms – where cannabis exposure enhances risk for psychosis in those with pre-existing genetic vulnerabilities – it could also be that cannabis use enhances risk for suicide only if certain pre-existing risk factors are present. Notably, however, the explanation cannot be simply that depressed adolescents are both more likely to have suicidal behaviors and to use cannabis, given that analyses controlled for the presence of a set of co-occurring mental health and substance use disorders including, but not limited to, depression. Future research should explore the co-occurrence of cannabis use disorder and suicidal behaviors, the extent to which cannabis use may be causally related to suicidal behavior, and the possible mechanisms underlying this linkage. This study indicates there is a strong association between cannabis use disorder and suicidal behaviors, which should be screened and addressed across clinical settings.
This study found that adolescents who were treated in an inpatient setting and had cannabis use disorder were much more likely to engage in suicidal behaviors. Furthermore, those with depression and cannabis use disorder were at an even higher risk of attempting suicide or self-harming than those with one or the other separately. Adolescence is an important stage of development during which key neurocognitive, social, and psychological changes occur. Suicide is a leading cause of death among this age group and cannabis is being perceived as less risky among youth in part due to cannabis legalization in many states. The study was cross-sectional and cannot determine if cannabis use and cannabis use disorder led to or caused suicidal behavior. It may be that suicidal behaviors and their underlying mechanisms were making cannabis use more likely. While future research may further examine whether cannabis use and suicidal behaviors are causally related, given their co-occurrence, screenings for suicide in adolescents may be improved by assessing for cannabis and screenings for cannabis use disorder in adolescents may be improved by assessing for suicide and self-harm.
Oladunjoye, A. F., Li, E., Aneni, K., & Onigu-Otite, E. (2023). Cannabis use disorder, suicide attempts, and self-harm among adolescents: A national inpatient study across the United States. PLOS ONE, 18(10), e0292922. doi: 10.1371/journal.pone.0292922