
Technology-enhanced contingency management: Exploring the feasibility
Only a subset of people with substance use disorder receive empirically-supported services. Developing and testing ways to get evidence-based treatments to more people may help bridge the divide between treatment need and receipt of services. In this study, researchers explored the feasibility of a digital contingency management intervention for substance use disorder delivered via a smartphone app which ultimately could reach many more people.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
There are millions of people in the United States every year who may benefit from substance use treatment but never receive care. Individuals seeking or needing treatment may experience a host of barriers such as stigma, personal attitude (e.g., thinking no one can help), readiness to change, financial access, and knowledge of where to go. Even when people recognize the need for treatment and may even receive care, 50% of people (median) report making 2 serious recovery attempts before resolving their substance use problem. The unmet need for treatment services and the variability in recovery attempts point to the need for accessible, effective treatments for substance use disorder.
Leveraging digital tools for substance use treatment may be able to complement formal treatment and improve individual recovery-related outcomes. Studies show that evidence-based in-person supports can be effectively translated into technology-based ones. Contingency management (CM) is among the most effective, evidence-based treatments for substance use disorders, and it has been shown to effectively reduce alcohol and tobacco use via mobile phone delivery.
Under contingency management interventions, prizes such as money are delivered to a participant dependent on objective evidence of drug abstinence. With recent advances in the accessibility of smartphones and drug testing supplies, there is an unprecedented opportunity to use this technology to deliver contingency management. In this study, researchers explored the feasibility of a new smartphone-delivered contingency management program to supplement standard care among adults with alcohol use disorder (AUD) enrolled in community-based outpatient substance use disorder (SUD) treatment.
HOW WAS THIS STUDY CONDUCTED?
This was a pilot randomized control trial (RCT) implemented to explore the feasibility and satisfaction among users with a digitally delivered contingency management intervention (DynamiCare Health) as a supplement to substance use disorder treatment among adults with alcohol use disorder.
The researchers recruited patients currently enrolled in outpatient substance use disorder treatment in the Boston/Cape Cod region (N = 61). Participants were randomly assigned to treatment as usual alone (n = 32) or treatment as usual combined with access to the contingency management app (n = 29) for a 90-day planned duration. Feasibility of the contingency management program was assessed by the number of days elapsed between first and last use of the app for submission of drug or alcohol tests. The number of tests and percent of requests that were completed was also evaluated. Feedback on the functionality of the app was also collected through a satisfaction survey.
All study participants were recruited from one of three outpatient substance use disorder clinics operated by the same organization. Most participants (n = 43) were enrolled in intensive outpatient group therapy. The remainder were enrolled in a short-term partial hospital program or individual counseling. The treatment as usual group (hereafter ‘control group’) continued to receive care as they would if not participating in this study. The experimental group continued to receive the same care but also had access to the contingency management app through which they were periodically promoted to self-conduct a breath or a saliva test.

At the beginning of the study, those in the experimental group participated in an orientation introducing the app where they learned how to take a photo/video of the test process and submit it for review. Tests had to be completed within 60 minutes of the request to be counted. Once submitted, off-site medical staff reviewed the testing procedure and results. If negative, monetary rewards were automatically uploaded onto a debit card. During the 90-day intervention period, tests were randomly requested 3-10 times per week (1-3 times per day) with 2-7 breath and 1-3 saliva tests. Consistent positive results triggered more frequent requests while consistent negative results triggered less frequent requests but with higher rewards. For each negative test, participants were rewarded 1-10 “coins” based on their consistency of negative results. Each “coin” value randomly ranged from $0 to $50, with an average of $1 per coin. Under the rewards schedule, each participant could earn a maximum of $600 over the 90-day period.
All participants were scheduled to complete monthly in-person assessments from baseline through 1 month after the planned intervention ended. In-person assessments consisted of questions about alcohol and drug use in the past 30 days and a 12-panel urinalysis. Participants could earn up to $100 for completion of all in-person assessments. Participants in the experimental were also sent a satisfaction survey.
The two study groups did not differ along demographics or baseline drug use. The sample was primarily White/Non-Hispanic (87%), mostly male (61%), and single (61%). Participants were on average 39.6 years old. The majority (67%) had at least a high school education with 59% reporting being currently employed at least part-time. Almost all the sample (89%) had Medicare or Medicaid or private insurance. A little over a third (38%) of the sample had undergone medically supervised withdrawal prior to entering the outpatient program, and 46% of the sample reported using alcohol or drugs in the last 30 days.
WHAT DID THIS STUDY FIND?
App utilization was substantial with high levels of compliance.
Among the experimental group that had access to the contingency management app, average duration of app use among the experimental group was 64 days. Among those that used the app for a least 7 days, they completed 68% of possible breath tests and 74% of possible saliva tests. The rate of compliance was not reported for the entire experimental group. Although all participants received an average of $248 in rewards, those using the app for at least 7 days earned an average of $287. Additionally, 38% of the whole group earned more than $400.

Of those in the experimental group who used the app for at least 7 days, 13 (45%) completed the utilization satisfaction survey 1-month post-randomization. These participants reported that many features of the app were helpful. Participants were also asked to indicate the component of their overall treatment experience that was most important. All respondents completing the survey endorsed the contingency management app; 77% selected self-help groups (e.g., AA and NA); and 62% indicated counseling.

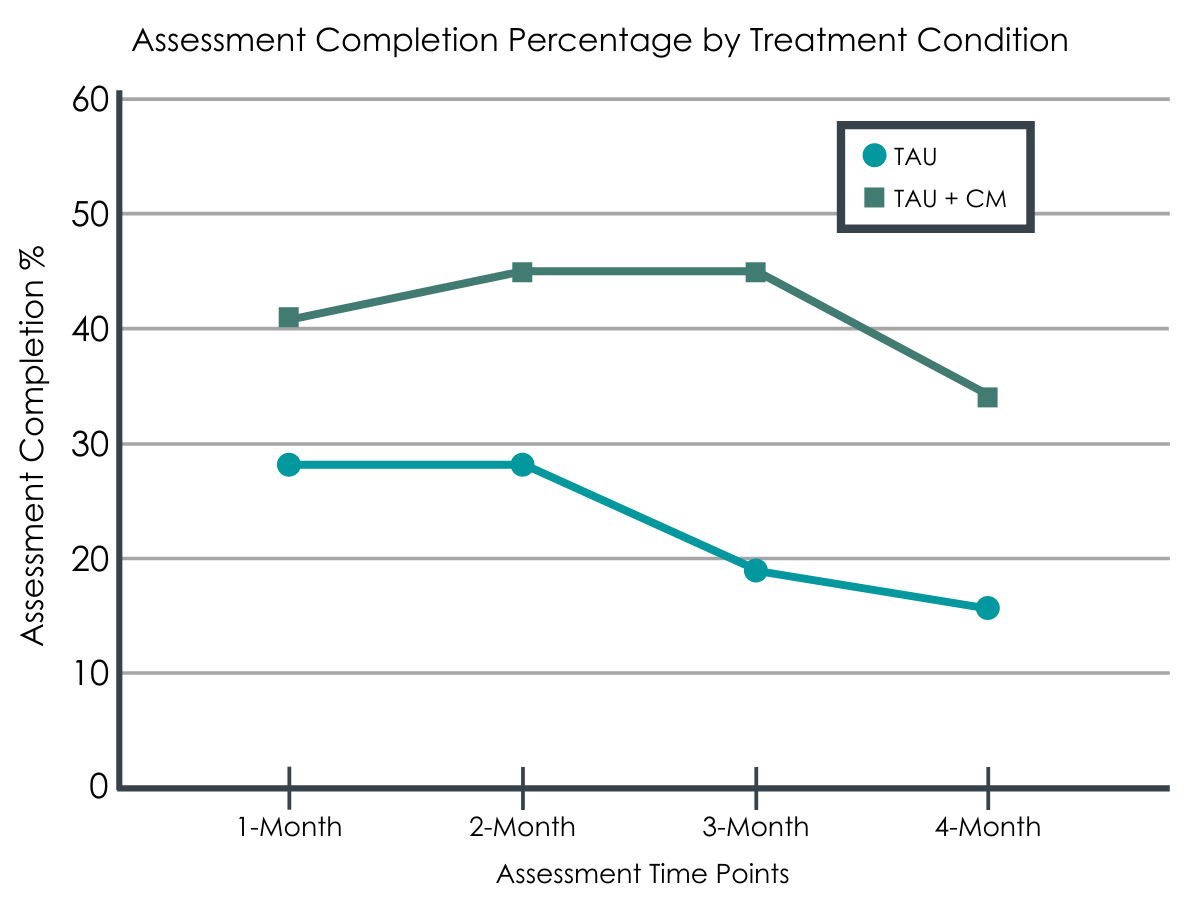
The experimental group completed more in-person assessments, but they did not attend treatment longer on average.
While the experimental group had a greater proportion still engaged in outpatient treatment 90 days after entering the study, they attended treatment a similar number of days relative to the control group.
In addition to pilot data on how individuals used the app, they also examined outcome differences among the conditions. Importantly, while participants in the experimental group (n = 29) showed up for the 1-, 2-, 3-, and 4- month in-person assessments more than those in the control group (n = 32), follow-up rates were very low overall among both groups. Specifically, the average in-person assessment completion rate was 41% among the experimental group and 23% among the control group. Considering missing tests as not confirmed abstinence, the overall rate of testing-confirmed abstinence from alcohol and non-prescribed drugs was 33% for those in the experimental group and 16% for the control group. However, the sample was too small and assessment completion too poor to attribute these differences to the contingency management app’s effectiveness.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
There is an acute need for accessible, effective substance use disorder treatments in the United States. Technological advancement and digital tools may increase access and allow for the implementation of some of the most effective in-person substance use disorder treatments. In this study, Hammond and colleagues provide preliminary evidence suggesting a digitally delivered contingency management program is feasible among a sample of adults with alcohol use disorder receiving outpatient treatment services. Most of the participants that had access to the contingency management app used the app for most of the treatment period. Among those who responded to the satisfaction survey, the app benefited their treatment experience. The frequency of app use and satisfaction with the app suggest that the remote delivery of a contingency management program may be suitable to deliver an effective contingency management intervention that adults would like to use.
Contingency management interventions, based on the psychological principals of operant conditioning, consist of applying positive reinforcements contingent upon behavior change. If a person successfully completes the desired behavior (e.g., abstinence), they are rewarded with a positive reinforcer (e.g., money). Meta-analyses have shown in-person contingency management produces clinically meaningful improvement in substance use. It may also enhance the effects of cognitive-behavioral therapy. The influence of contingency management on substance use outcomes may also vary along sociodemographic and health factors. For example, those with previous substance use treatment have a stronger positive response to contingency management than those without a treatment history. Similarly, those with higher psychiatric severity experience greater benefits from contingency management. However, risk-takers experience less beneficial effects of contingency management. Because of the generally positive effects of contingency management interventions, it is an ideal intervention to be translated into an automated, digital delivery system.
Automated, digital delivery of a contingency management program offers numerous benefits:
- It increases access to the intervention by allowing it to be delivered without the need for recurrent attendance at in-person clinical services.
- The randomization algorithms of testing enabled by digitally delivered contingency management also reduces a participant’s ability to guess when a test will be requested and establishes a stronger link between behavior and reward.
- The ability to remotely complete either a breath or saliva test allows a person to go about their normal daily activities and still be compliant.
- Remote testing and intervention implementation mitigates in-person risks, such as the transmission and/or spread of COVID-19.
While studies like these show technology-based contingency management is feasible, it has yet to be shown empirically if digitally delivered automated contingency management is as effective as the in-person version across all substances and recovery outcomes. Existing evidence does suggest that automated contingency management may reduce barriers and improve treatment outcomes. For example, those with opioid use disorder (OUD) and those seeking smoking cessation participating in digital contingency management programs have had improved short-term abstinence rates compared with their respective control conditions.
The researchers in this study present the use of a novel digital contingency management tool, future investigation will need to consider the feasibility of scaling up such programs. Secondary analysis of contingency management programs shows it may be cost-effective for community health center-based outpatient programs. The willingness of providers to recommend contingency management and the likelihood that insurance companies will reimburse its cost remains unknown.
Future investigation may benefit from a large-scale feasibility study and exploring insurers’ perspectives in paying for contingency management. Furthermore, the cost of licensing specific contingency management programs, such as the one assessed in this study, is not known and will likely influence its use. Regardless, this pilot study suggests that a contingency management program can be automated and delivered digitally with high utilization and compliance.
- LIMITATIONS
-
- The sample of participants was small and demographically similar, which limits the generalizability of these findings.
- In-person assessment completion was low for both groups but especially so for the treatment as usual group. Poor completion rates prevent the researchers from making valid and reliable claims about substance use outcomes, including comparing the two groups.
- The app usage satisfaction survey also had a low response rate, which may introduce selection bias – those participants who completed the survey may have been more likely to report it as beneficial compared to those that did not complete it.
- Feedback from the app usage satisfaction survey were all positive. Future exploration of programmatic or digital aspects that could be improved is warranted.
- The researchers and the development of the licensed app software was funded in part by the NIH/NIAAA Small Business Innovative Research and Small Business Technology Transfer Grant (1R43AA026234-01), which may introduce bias towards reporting on the most favorable results. However, the authors are not employed by DynamiCare, and the authors had “no conflicts of interest to disclose.”
BOTTOM LINE
Researchers in this randomized control trial found that adults enrolled in outpatient substance use disorder treatment around the Boston/Cape Cod area had high utilization of a digitally delivered automated contingency management app and perceived it as beneficial for their treatment goals. Although the research team present substance use outcomes, the small sample and low in-person assessment completion rates prevent conclusions about the efficacy of adding a digital contingency management intervention to outpatient treatment. If future researchers investigate digital contingency management programs compared to in-person ones, they may be able to determine any relative differences and for whom digital interventions may be most beneficial. If these findings are consistent with in-person treatment effects, then digital contingency management programs may increase access to treatment, improve treatment adherence and substance use outcomes, and reduce the time and cost of in-person program facilitation. These findings, however, should be treated as important hypotheses to be tested in the future.
- For individuals and families seeking recovery: The researchers from this study explore if turning one of the most effective treatments for substance use disorder – contingency management – into an automated, digital tool is possible. They find that early evidence points to yes. Although it may sound counterintuitive to reward someone with money to be abstinent, contingency management has been shown to be an effective applied behavioral change strategy. Rewards can be linked to a debit card that prevents its use at potentially problematic outlets such as liquor stores. Developing a digital tool to deliver such a intervention may help increase access and treatment adherence. If you or a loved one is invited to participate in a digitally delivered contingency management program, it is unlikely to harm and it may help achieve treatment goals.
- For treatment professionals and treatment systems: Contingency management has been suggested and tested for over 50 years in behavioral and clinical psychology. The advent and accessibility of digital tools, however, is more recent. Although contingency management is a proven method for improving treatment outcomes, the translation of it into an automated digital tool has not been fully tested. The researchers from this study present pilot findings that one such digital tool is feasible and satisfactory for adults already receiving outpatient treatment for substance use disorder. Subject to future investigation, digital contingency management may be a beneficial supplement to standard treatment.
- For scientists: This study and others like it demonstrate the feasibility of digital contingency management programs, which may improve access and treatment outcomes simultaneously. However, more work is needed to determine the comparative effectiveness of these digital platforms as well as longer-term benefits of contingency management. More work is also needed to probe the underlying mechanisms of technology-based interventions as well as the potential opportunity cost of forgoing face-to-face provider-participant interactions. Furthermore, the private-public-academic partnerships in software development and treatment implementation may be beneficial to those with substance use disorder. Additional comparative analysis is needed to tease apart group differences.
- For policy makers: More research is needed to establish the treatment benefits of a digital contingency management tool, but this study suggests such a tool is feasible and well-received by participants. Although a digital contingency management program may represent a significant cost to health-care providers up front, the treatment benefits and cost effectiveness of contingency management are substantial. Supporting the development of digital tools to implement contingency management will likely improve access to one of the most effective treatments for substance use disorder.
CITATIONS
Hammond, A. S., Sweeney, M. M., Chikosi, T. U., & Stitzer, M. L. (2021). Digital delivery of a contingency management intervention for substance use disorder: A feasibility study with DynamiCare Health. Journal of Substance Abuse Treatment, 126, 108425. doi: 10.1016/j.jsat.2021.108425