Imagine hurling your favorite drink away from you: A new technique reduces alcohol craving
Craving alcohol is a core symptom of alcohol use disorder and an important target for recovery. Given most people with alcohol use disorder do not seek treatment, easy and appealing interventions may help more people initiate recovery. This randomized controlled trial examined a unique, brief treatment for alcohol use disorder that used imagined experiences and movements to help override an individual’s urge to drink.
Craving alcohol is a core symptom of alcohol use disorder and an important target for treatment. Although there are many useful psychological and pharmacological interventions, relapse rates remain high. As treatment seeking and engagement in treatment are relatively low, researchers have called for appealing strategies that are convenient and accessible.
A relatively new line of treatment for alcohol use disorder aims at overriding the urge to consume alcohol by changing implicit cognitions through a technique called “approach bias modification.” Implicit cognitions can be described as influences occurring outside one’s conscious awareness such as knowledge, perception, or memory, that influence a person’s behavior.
Implicit cognitions are one potential explanation behind why a person with alcohol use disorder may have the inability to resist the urge to drink. Though initial alcohol or other drug taking may be a fully conscious choice, recent studies have shown that automatic processes play a large role in the development of addiction and the high risk of relapse. That is, there is evidence that drug cues (i.e., reminders in the environment, such as a cocktail glass or the smell of an alcoholic drink) capture automatic attention, evoke activation in the midbrain’s dopamine reward system and engender automatic approach responses making it more likely someone would consume alcohol among individuals with an alcohol or other drug use disorder, each of which may take place largely outside of conscious awareness. These automatically activated processes have been associated with increased alcohol or other drug consumption, despite the fact that individuals may express an explicit wish to quit.
Implicit approach or avoidance reactions are not limited to alcohol or other drug use among individuals who drink or use drugs. Approach/avoidance tendencies may be general bodily reactions to positive and negative stimuli that all people experience. This has been shown in prior research with positive and negative words, fear of spiders, smiling vs. angry faces among individuals with social anxiety, muted reactions in depressed patients vs. non-depressed controls, and more limited approach bias in patients with anorexia nervosa compared to controls. This research tests approach/avoidance tendencies through computerized training paradigms, where, an individual is asked to push away an image or pull the image towards themselves, using a joy stick or button press, for example, and their reaction time is recorded. Shorter reaction times are considered more automatic whereas longer reaction times are considered more controlled. For example, a person with a fear of spiders had a shorter reaction time when asked to push the picture of a spider away with a joy stick than when asked to pull the picture towards them, compared to individuals without a fear of spiders.
Approach bias modification is one type in a set of procedures in psychology called “cognitive bias modification” that aim to directly change these automatic, unconscious tendencies to behave in a certain way in the presence of a particular cue (in this case, alcohol) through repeated practice of a new behavior while imagining or viewing that particular cue (for example, picturing a drink in your mind or looking at a picture of a drink). These procedures are often used the in the treatment of certain anxiety-related disorders, such as nail-biting, skin-picking or hair pulling, where the participant is to practice several times a day the same bodily motion to begin the target behavior, such as bringing their finger to their mouth to bite their nail, then redirecting their body somewhere else, such as touching their finger to their ear. This is practiced over and over to change the automatic behavior that happens outside the person’s conscious awareness. For drinking, this may look like asking a participant to imagine hurling their favorite alcoholic beverage(s) away from themselves; the throwing motion is performed, but the beverage and the situation are only imagined.
In the current study, the researchers conducted a randomized controlled trial testing a brief approach bias modification-based intervention to reduce alcohol craving among adults seeking to reduce problematic drinking.
HOW WAS THIS STUDY CONDUCTED?
This online randomized controlled experiment examined the efficacy of a brief behavioral treatment technique to reduce alcohol craving among (N = 227) adults seeking to reduce problematic drinking.
Participants were recruited online using a participant pool of German-speaking people who have registered for participation in web-based studies. The only inclusion criterion was participants’ self-reported desire to reduce problematic alcohol consumption. Severity of drinking behavior was assessed with a commonly used measure of alcohol use and problems (the 10-item Alcohol Use Disorders Identification Test [AUDIT]).
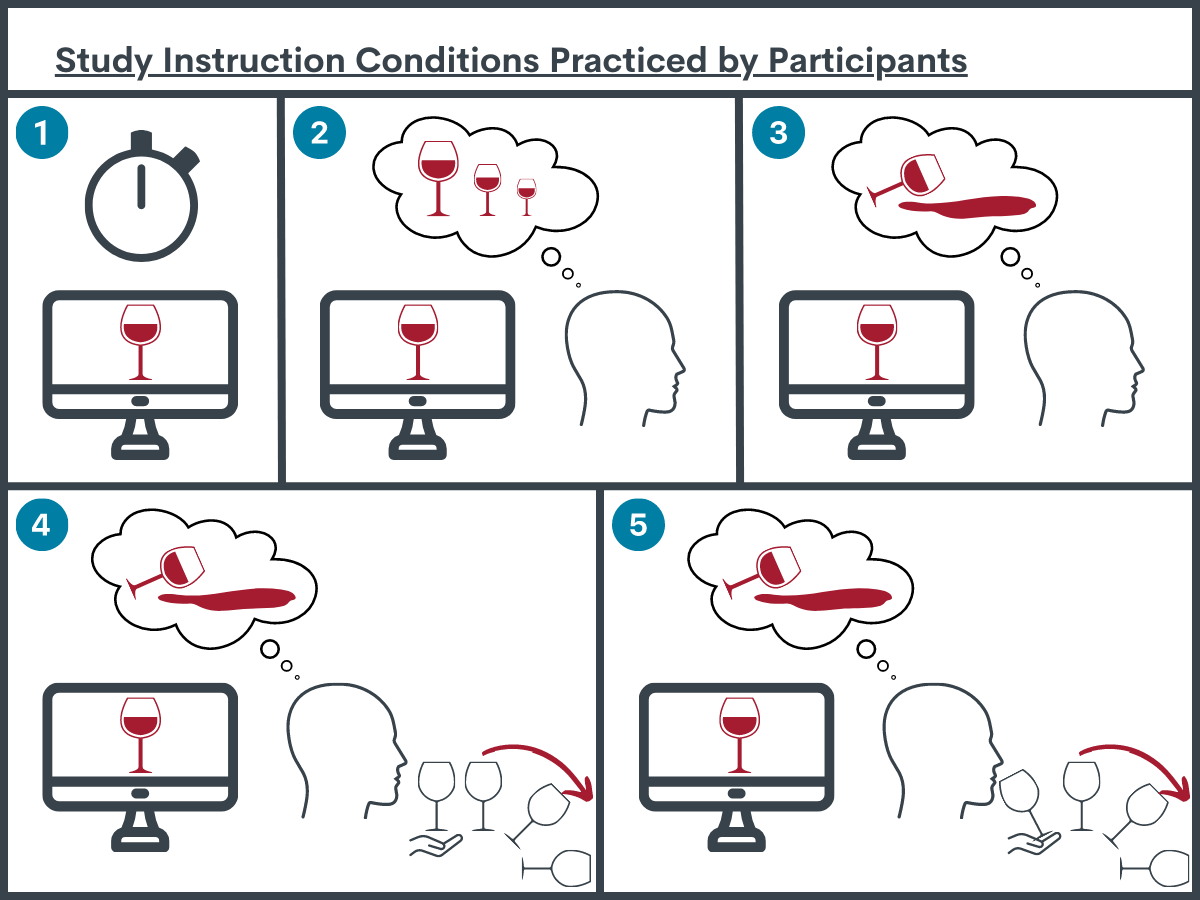
Participants were asked to rate their current level of craving for alcohol (primary outcome) on a scale ranging from 0 (not at all) to 100 (extreme) after viewing the same three pictures of alcohol cues. Participants were then randomized to 1 out of 5 conditions. Each participant was shown the same photo of a hand holding a full wine glass. Then were given one of the following instructions:
Wait-list control condition: Look at the photo for some time
Zooming-out condition: Make the photo smaller in your imagination (a standardfeature of approach bias modification procedures)
Imaginal retraining without movement condition: Imagine pouring out the liquid or throwing the glass away without making the actual movement
Imaginal retraining condition with movement: Imagine pouring out the liquid or throwing the glass away while making the actual movement
3P (pull-pause-push) condition: Imagine bringing the glass close to your mouth, stopping just short of your mouth, and then pour out the (imagined) liquid or throw the glass away while making the actual movement
In conditions 2-5, participants were asked to perform the exercise at least 5 times; general instructions were essentially the same. After the intervention, participants were asked whether they had actually executed the task, and had to indicate their current level of craving for alcohol on a scale from 0 to 100.
The analysis compared participants’ changes in craving from pre- to post-assessment across the 5 intervention conditions. The researchers ran the same analyses with all participants and again with only the participants who reported they had performed the exercises as instructed (i.e., a “sensitivity analysis”), which was the case for 91.2% of the sample. Participants adhered to the intervention instructions equally across conditions. Both analyses yielded the same pattern of results. In follow-up analyses, they tested if there were differences in intervention effects for participants with higher craving at baseline or other demographic or clinical characteristics.
Slightly more men than women participated (53.7% vs.46.3%). On average, participants were on average in their mid-50s. Approximately one third (32.6%) of the participants had not finished high school. On a commonly used measure of alcohol use and problems, most participants scored in the hazardous or harmful drinking range; 33% were in the alcohol-dependent range (i.e., moderate to severe DSM 5 alcohol use disorder). Intervention condition groups differed on gender and age, where fewer women in conditions 1 (37.2%) and 3 (28.6%) compared to conditions 2 (50%), 4 (53.5%), and 5 (63%), and participants were slightly older in conditions 3 (average 60 years old) and 5 (average 59 years old), and slightly younger in condition 4 (average 49 years old), compared to conditions 1 and 2 where participants were 52 and 54 years old on average, respectively. Groups did not differ on baseline levels of craving, alcohol use and problem severity, depression symptoms, education, nor work status.
WHAT DID THIS STUDY FIND?
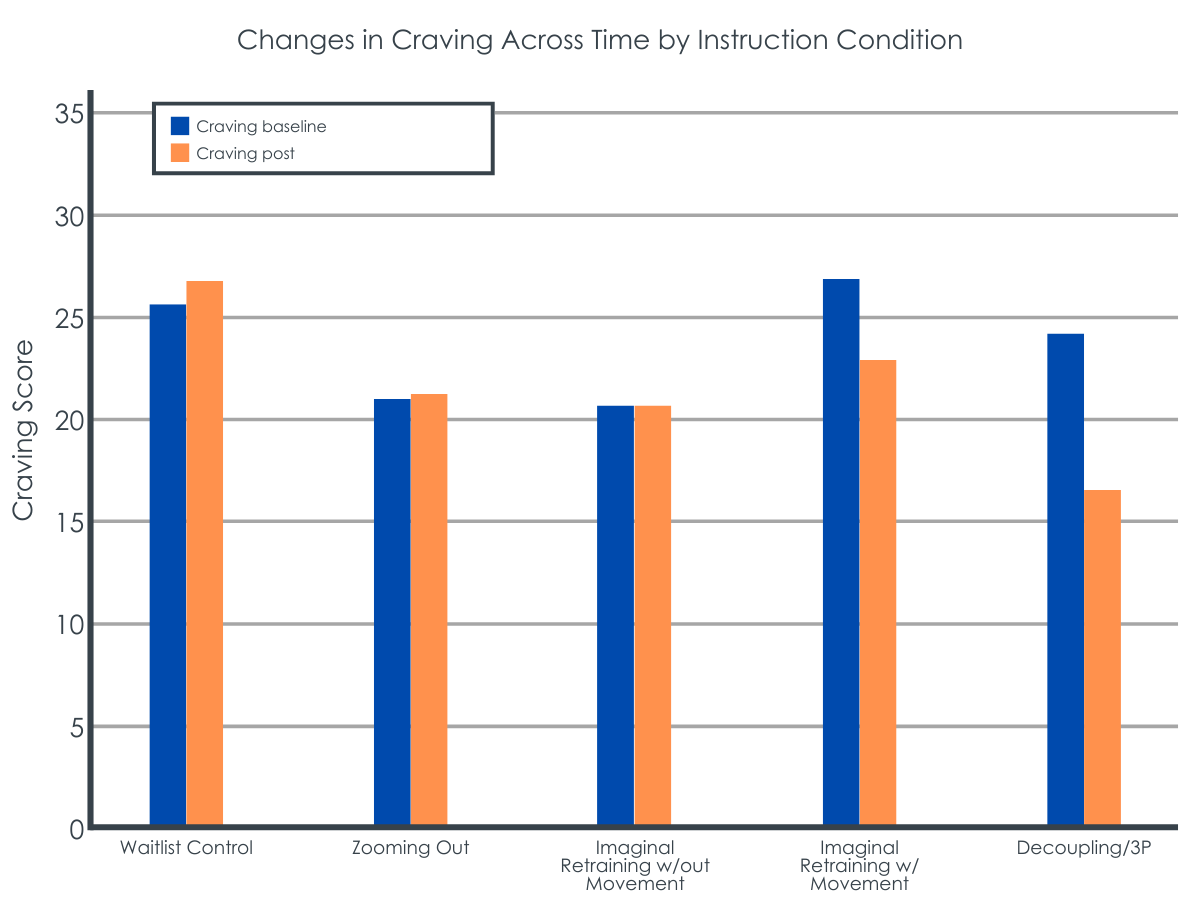
Only the 3P condition lessened craving by approximately 1/3.
Alcohol craving did not change in the wait-list control condition, zooming-out condition, imaginal retraining without movement condition, or the imaginal retraining with movement condition. Only the 3P condition lessened craving (by 35%), which was a medium-sized effect.
Participants in the 3P group with high craving benefited the most from the intervention relative to those participants in conditions 1-3.
Participants with higher craving in the 3P condition showed a stronger decline in craving compared to those in the wait-list control, zooming out, and imaginal retraining without movement conditions. It makes sense that participants with the highest cravings had the greatest decline because it is a natural tendency for an extreme state of being to revert back to the middle or average over time (i.e., regress to the mean). Importantly, age and gender, where some group differences emerged, did not influence the effect of the intervention on craving. And, alcohol use problem severity at baseline did not influence the effect of the intervention on craving.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This randomized controlled experiment showed that an intervention focused on changing implicit cognitions through approach bias modification techniques can reduce self-reported alcohol craving among adults seeking to reduce problematic drinking. Specifically, combining two techniques commonly used in treatments for nail-biting, skin-picking, and hair-pulling, i.e. “imaginal retraining” (imagining the alcoholic drink getting smaller, being poured out, or thrown away from you) and “decoupling” (actually practicing the movement of pouring out the drink or pushing it away from you after bringing the drink close to your mouth) was the only variation of treatment that produced a change in alcohol craving ratings compared to imaginal retraining techniques alone or wait-list control.
The researchers have tested imaginal retraining techniques (without decoupling) before to reduce cravings in several domains including: problematic alcohol use; tobacco smoking; and eating among overweight individuals. In similar randomized controlled experiments, imaginal retraining reduced craving for alcohol and self-reported alcohol use, reduced craving for cigarettes and self-reported cigarette smoking, and reduced craving for high-caloric foods and produced greater weight loss. However, in each of these studies including the current study, outcomes were based on self-report and participants were recruited online. Future research with objective measures, such as blood or urine toxicology test verification to confirm alcohol or other drug use, is needed to confirm that reduced craving actually leads to reduced use after these treatment approaches. Also, it is unclear how long such an effect may last and what optimal “dose” or intensity may be needed; it may be that the effect is short-lived and it may need repeating. Different intensities and durations may be needed for different individuals across time. More study is needed in these regards with this specific approach and how it may compare to other similar methods.
Other approach bias modification techniques also show promising outcomes for adults with alcohol use disorder. One study tested an approach bias modification technique using a joystick where you push an image of a drink away from you. Participants completed 4 sessions of the technique before entering inpatient treatment for alcohol use disorder and showed immediate changes in reactivity towards alcohol cues. Those who completed 4 sessions of the technique also had better treatment outcomes one year later. In another study from the same researchers, participants in inpatient treatment for alcohol use disorder showed that reduced craving after completing a similar bias modification technique was associated with reduced activation in the amygdala.
A compelling component of the current intervention is how quick, simple, and easy it would be to implement, especially compared to other bias modification techniques using additional technical equipment, like joy sticks for example. All a person would need is to find a quiet space to imagine the drink (or other subject of craving) and perform the movement (bring the imagined drink up to your mouth and throw it away from you). Given that so few people experiencing alcohol problems access formal care, brief and easy to implement skills like the intervention tested here are so valuable in that they provide more real-time strategies to cope with cravings.
This randomized controlled study provides a jumping off point for further research developing new, brief, and easy to implement treatments for alcohol and other drug use disorders. Future research would need to test the efficacy of this intervention over time, and as well as understand if and how this could be incorporated into various substance use treatment settings. As noted above, for example, how long does this technique reduce cravings? Does craving reduction produced by this technique translate to actual reduced drinking? Who, in particular, is more or less likely to respond? Who would deliver this intervention and in what settings? Could it be used as a self-help mobile app? More research in this line of work is needed to understand how using a technique like this in real-life could reduce craving, and potentially subsequently reduce alcohol use and related harms. If found to be effective, a simple intervention like this could potentially be easily adopted by a large number of people seeking to reduce alcohol craving.
Participants were recruited online by self-reported desire to reduce problematic drinking, and there was no assessment of alcohol use disorder. Future research should verify participants meet criteria for alcohol use disorder to confirm the intervention produces the same effects in a treatment target population.
Since the experimental research was performed exclusively online, it is difficult to know how generalizable the results are to a real-world setting. The researchers simply asked participants if they performed the technique, where participants could simply respond ‘Yes’ or ‘No’ on the survey, with no other way to determine if participants actually did, in fact, perform the technique. This doesn’t provide the researchers an objective, reliable way to determine how faithfully participants adhered to the intended intervention protocol or if they completed it at all. Future research should include more rigorous evaluations of this bias modification skill (e.g., video of participants performing the throwing motion), to have a more accurate understanding of how this could affect craving, especially in naturalistic settings.
BOTTOM LINE
This study found that among 227 adults seeking to reduce problematic alcohol use recruited online in Germany that a new behavioral treatment technique grounded in cognitive bias modification reduced immediate subjective cravings for alcohol by 1/3 compared to active control. Though more research examining this particular approach with more rigorous designs and in different samples can help determine its ultimate utility, cognitive bias modification interventions seem a promising new area for further exploration in the treatment of alcohol and other drug use disorders.
For individuals and families seeking recovery: Implicit cognition is a possible explanation for a common experience described by some people with alcohol use disorder where they have lost the ability to resist the urge to drink – drinking becomes automatic. This new, brief, and convenient behavioral treatment technique aims to change implicit cognitions by having the person imagine hurling their favorite alcoholic beverage(s) away from themselves – the movement is actually performed, but the beverage and the situation are only imagined – and showed immediate reductions in craving after performing the technique. Future research is needed to understand how long such an effect may last and if this actually translates to reduced drinking, and how it could be incorporated into treatment.
For treatment professionals and treatment systems: Although effective alcohol use interventions are available, relapse rates remain high. Approach bias modification techniques used to treat nail-biting, hair-pulling, and skin-picking are new area for exploration in the treatment of addictive behaviors. Imaginal retraining and decoupling when combined showed immediate reductions in alcohol craving. Future research is needed to understand if this technique actually translates to reduced drinking, how long any therapeutic effects may last, for whom in particular it may be helpful or unhelpful, and how it could be incorporated into treatment for alcohol or other drug use disorders.
For scientists:This randomized controlled experiment conducted online with (N = 227) German-speaking adults with a self-reported desire to reduce problematic alcohol consumption showed that a new approach bias modification technique called 3P (pull-pause-push) reduced immediate subjective ratings of alcohol craving compared to active control. 3P combines imaginal retraining and decoupling, a similar approach to treating body-focused repetitive behaviors (e.g., nail-biting, hair-pulling, and skin-picking). 3P produced greater reductions in craving compared to imaginal retraining alone and wait-list control. Moderation analyses showed a treatment by craving interaction effect, such that participants with high baseline craving ratings benefitted most from the 3P intervention, but this may partly an effect or regression to the mean artifact. Other baseline characteristics, such as age, gender, and alcohol use problem severity did not moderate the effect of treatment on changes in craving. Future research with verified alcohol use disorder and objective measures of changes in drinking are needed to understand the efficacy of this technique for alcohol use disorder treatment.
For policy makers: Although effective alcohol use interventions are available, relapse rates remain high. As treatment seeking and engagement in treatment are relatively low, researchers have called for new, appealing interventions that are brief and convenient. Craving alcohol is a core symptom of alcohol use disorder and an important target for treatment. A new behavioral intervention technique showed immediate reductions in alcohol craving. Future research is needed to understand if this technique actually translates to reduced drinking, how long any observed therapeutic effect may last, and how it could be incorporated into treatment for alcohol or other drug use disorders.
Craving alcohol is a core symptom of alcohol use disorder and an important target for treatment. Although there are many useful psychological and pharmacological interventions, relapse rates remain high. As treatment seeking and engagement in treatment are relatively low, researchers have called for appealing strategies that are convenient and accessible.
A relatively new line of treatment for alcohol use disorder aims at overriding the urge to consume alcohol by changing implicit cognitions through a technique called “approach bias modification.” Implicit cognitions can be described as influences occurring outside one’s conscious awareness such as knowledge, perception, or memory, that influence a person’s behavior.
Implicit cognitions are one potential explanation behind why a person with alcohol use disorder may have the inability to resist the urge to drink. Though initial alcohol or other drug taking may be a fully conscious choice, recent studies have shown that automatic processes play a large role in the development of addiction and the high risk of relapse. That is, there is evidence that drug cues (i.e., reminders in the environment, such as a cocktail glass or the smell of an alcoholic drink) capture automatic attention, evoke activation in the midbrain’s dopamine reward system and engender automatic approach responses making it more likely someone would consume alcohol among individuals with an alcohol or other drug use disorder, each of which may take place largely outside of conscious awareness. These automatically activated processes have been associated with increased alcohol or other drug consumption, despite the fact that individuals may express an explicit wish to quit.
Implicit approach or avoidance reactions are not limited to alcohol or other drug use among individuals who drink or use drugs. Approach/avoidance tendencies may be general bodily reactions to positive and negative stimuli that all people experience. This has been shown in prior research with positive and negative words, fear of spiders, smiling vs. angry faces among individuals with social anxiety, muted reactions in depressed patients vs. non-depressed controls, and more limited approach bias in patients with anorexia nervosa compared to controls. This research tests approach/avoidance tendencies through computerized training paradigms, where, an individual is asked to push away an image or pull the image towards themselves, using a joy stick or button press, for example, and their reaction time is recorded. Shorter reaction times are considered more automatic whereas longer reaction times are considered more controlled. For example, a person with a fear of spiders had a shorter reaction time when asked to push the picture of a spider away with a joy stick than when asked to pull the picture towards them, compared to individuals without a fear of spiders.
Approach bias modification is one type in a set of procedures in psychology called “cognitive bias modification” that aim to directly change these automatic, unconscious tendencies to behave in a certain way in the presence of a particular cue (in this case, alcohol) through repeated practice of a new behavior while imagining or viewing that particular cue (for example, picturing a drink in your mind or looking at a picture of a drink). These procedures are often used the in the treatment of certain anxiety-related disorders, such as nail-biting, skin-picking or hair pulling, where the participant is to practice several times a day the same bodily motion to begin the target behavior, such as bringing their finger to their mouth to bite their nail, then redirecting their body somewhere else, such as touching their finger to their ear. This is practiced over and over to change the automatic behavior that happens outside the person’s conscious awareness. For drinking, this may look like asking a participant to imagine hurling their favorite alcoholic beverage(s) away from themselves; the throwing motion is performed, but the beverage and the situation are only imagined.
In the current study, the researchers conducted a randomized controlled trial testing a brief approach bias modification-based intervention to reduce alcohol craving among adults seeking to reduce problematic drinking.
HOW WAS THIS STUDY CONDUCTED?
This online randomized controlled experiment examined the efficacy of a brief behavioral treatment technique to reduce alcohol craving among (N = 227) adults seeking to reduce problematic drinking.
Participants were recruited online using a participant pool of German-speaking people who have registered for participation in web-based studies. The only inclusion criterion was participants’ self-reported desire to reduce problematic alcohol consumption. Severity of drinking behavior was assessed with a commonly used measure of alcohol use and problems (the 10-item Alcohol Use Disorders Identification Test [AUDIT]).
Participants were asked to rate their current level of craving for alcohol (primary outcome) on a scale ranging from 0 (not at all) to 100 (extreme) after viewing the same three pictures of alcohol cues. Participants were then randomized to 1 out of 5 conditions. Each participant was shown the same photo of a hand holding a full wine glass. Then were given one of the following instructions:
Wait-list control condition: Look at the photo for some time
Zooming-out condition: Make the photo smaller in your imagination (a standardfeature of approach bias modification procedures)
Imaginal retraining without movement condition: Imagine pouring out the liquid or throwing the glass away without making the actual movement
Imaginal retraining condition with movement: Imagine pouring out the liquid or throwing the glass away while making the actual movement
3P (pull-pause-push) condition: Imagine bringing the glass close to your mouth, stopping just short of your mouth, and then pour out the (imagined) liquid or throw the glass away while making the actual movement
In conditions 2-5, participants were asked to perform the exercise at least 5 times; general instructions were essentially the same. After the intervention, participants were asked whether they had actually executed the task, and had to indicate their current level of craving for alcohol on a scale from 0 to 100.
The analysis compared participants’ changes in craving from pre- to post-assessment across the 5 intervention conditions. The researchers ran the same analyses with all participants and again with only the participants who reported they had performed the exercises as instructed (i.e., a “sensitivity analysis”), which was the case for 91.2% of the sample. Participants adhered to the intervention instructions equally across conditions. Both analyses yielded the same pattern of results. In follow-up analyses, they tested if there were differences in intervention effects for participants with higher craving at baseline or other demographic or clinical characteristics.
Slightly more men than women participated (53.7% vs.46.3%). On average, participants were on average in their mid-50s. Approximately one third (32.6%) of the participants had not finished high school. On a commonly used measure of alcohol use and problems, most participants scored in the hazardous or harmful drinking range; 33% were in the alcohol-dependent range (i.e., moderate to severe DSM 5 alcohol use disorder). Intervention condition groups differed on gender and age, where fewer women in conditions 1 (37.2%) and 3 (28.6%) compared to conditions 2 (50%), 4 (53.5%), and 5 (63%), and participants were slightly older in conditions 3 (average 60 years old) and 5 (average 59 years old), and slightly younger in condition 4 (average 49 years old), compared to conditions 1 and 2 where participants were 52 and 54 years old on average, respectively. Groups did not differ on baseline levels of craving, alcohol use and problem severity, depression symptoms, education, nor work status.
WHAT DID THIS STUDY FIND?
Only the 3P condition lessened craving by approximately 1/3.
Alcohol craving did not change in the wait-list control condition, zooming-out condition, imaginal retraining without movement condition, or the imaginal retraining with movement condition. Only the 3P condition lessened craving (by 35%), which was a medium-sized effect.
Participants in the 3P group with high craving benefited the most from the intervention relative to those participants in conditions 1-3.
Participants with higher craving in the 3P condition showed a stronger decline in craving compared to those in the wait-list control, zooming out, and imaginal retraining without movement conditions. It makes sense that participants with the highest cravings had the greatest decline because it is a natural tendency for an extreme state of being to revert back to the middle or average over time (i.e., regress to the mean). Importantly, age and gender, where some group differences emerged, did not influence the effect of the intervention on craving. And, alcohol use problem severity at baseline did not influence the effect of the intervention on craving.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This randomized controlled experiment showed that an intervention focused on changing implicit cognitions through approach bias modification techniques can reduce self-reported alcohol craving among adults seeking to reduce problematic drinking. Specifically, combining two techniques commonly used in treatments for nail-biting, skin-picking, and hair-pulling, i.e. “imaginal retraining” (imagining the alcoholic drink getting smaller, being poured out, or thrown away from you) and “decoupling” (actually practicing the movement of pouring out the drink or pushing it away from you after bringing the drink close to your mouth) was the only variation of treatment that produced a change in alcohol craving ratings compared to imaginal retraining techniques alone or wait-list control.
The researchers have tested imaginal retraining techniques (without decoupling) before to reduce cravings in several domains including: problematic alcohol use; tobacco smoking; and eating among overweight individuals. In similar randomized controlled experiments, imaginal retraining reduced craving for alcohol and self-reported alcohol use, reduced craving for cigarettes and self-reported cigarette smoking, and reduced craving for high-caloric foods and produced greater weight loss. However, in each of these studies including the current study, outcomes were based on self-report and participants were recruited online. Future research with objective measures, such as blood or urine toxicology test verification to confirm alcohol or other drug use, is needed to confirm that reduced craving actually leads to reduced use after these treatment approaches. Also, it is unclear how long such an effect may last and what optimal “dose” or intensity may be needed; it may be that the effect is short-lived and it may need repeating. Different intensities and durations may be needed for different individuals across time. More study is needed in these regards with this specific approach and how it may compare to other similar methods.
Other approach bias modification techniques also show promising outcomes for adults with alcohol use disorder. One study tested an approach bias modification technique using a joystick where you push an image of a drink away from you. Participants completed 4 sessions of the technique before entering inpatient treatment for alcohol use disorder and showed immediate changes in reactivity towards alcohol cues. Those who completed 4 sessions of the technique also had better treatment outcomes one year later. In another study from the same researchers, participants in inpatient treatment for alcohol use disorder showed that reduced craving after completing a similar bias modification technique was associated with reduced activation in the amygdala.
A compelling component of the current intervention is how quick, simple, and easy it would be to implement, especially compared to other bias modification techniques using additional technical equipment, like joy sticks for example. All a person would need is to find a quiet space to imagine the drink (or other subject of craving) and perform the movement (bring the imagined drink up to your mouth and throw it away from you). Given that so few people experiencing alcohol problems access formal care, brief and easy to implement skills like the intervention tested here are so valuable in that they provide more real-time strategies to cope with cravings.
This randomized controlled study provides a jumping off point for further research developing new, brief, and easy to implement treatments for alcohol and other drug use disorders. Future research would need to test the efficacy of this intervention over time, and as well as understand if and how this could be incorporated into various substance use treatment settings. As noted above, for example, how long does this technique reduce cravings? Does craving reduction produced by this technique translate to actual reduced drinking? Who, in particular, is more or less likely to respond? Who would deliver this intervention and in what settings? Could it be used as a self-help mobile app? More research in this line of work is needed to understand how using a technique like this in real-life could reduce craving, and potentially subsequently reduce alcohol use and related harms. If found to be effective, a simple intervention like this could potentially be easily adopted by a large number of people seeking to reduce alcohol craving.
Participants were recruited online by self-reported desire to reduce problematic drinking, and there was no assessment of alcohol use disorder. Future research should verify participants meet criteria for alcohol use disorder to confirm the intervention produces the same effects in a treatment target population.
Since the experimental research was performed exclusively online, it is difficult to know how generalizable the results are to a real-world setting. The researchers simply asked participants if they performed the technique, where participants could simply respond ‘Yes’ or ‘No’ on the survey, with no other way to determine if participants actually did, in fact, perform the technique. This doesn’t provide the researchers an objective, reliable way to determine how faithfully participants adhered to the intended intervention protocol or if they completed it at all. Future research should include more rigorous evaluations of this bias modification skill (e.g., video of participants performing the throwing motion), to have a more accurate understanding of how this could affect craving, especially in naturalistic settings.
BOTTOM LINE
This study found that among 227 adults seeking to reduce problematic alcohol use recruited online in Germany that a new behavioral treatment technique grounded in cognitive bias modification reduced immediate subjective cravings for alcohol by 1/3 compared to active control. Though more research examining this particular approach with more rigorous designs and in different samples can help determine its ultimate utility, cognitive bias modification interventions seem a promising new area for further exploration in the treatment of alcohol and other drug use disorders.
For individuals and families seeking recovery: Implicit cognition is a possible explanation for a common experience described by some people with alcohol use disorder where they have lost the ability to resist the urge to drink – drinking becomes automatic. This new, brief, and convenient behavioral treatment technique aims to change implicit cognitions by having the person imagine hurling their favorite alcoholic beverage(s) away from themselves – the movement is actually performed, but the beverage and the situation are only imagined – and showed immediate reductions in craving after performing the technique. Future research is needed to understand how long such an effect may last and if this actually translates to reduced drinking, and how it could be incorporated into treatment.
For treatment professionals and treatment systems: Although effective alcohol use interventions are available, relapse rates remain high. Approach bias modification techniques used to treat nail-biting, hair-pulling, and skin-picking are new area for exploration in the treatment of addictive behaviors. Imaginal retraining and decoupling when combined showed immediate reductions in alcohol craving. Future research is needed to understand if this technique actually translates to reduced drinking, how long any therapeutic effects may last, for whom in particular it may be helpful or unhelpful, and how it could be incorporated into treatment for alcohol or other drug use disorders.
For scientists:This randomized controlled experiment conducted online with (N = 227) German-speaking adults with a self-reported desire to reduce problematic alcohol consumption showed that a new approach bias modification technique called 3P (pull-pause-push) reduced immediate subjective ratings of alcohol craving compared to active control. 3P combines imaginal retraining and decoupling, a similar approach to treating body-focused repetitive behaviors (e.g., nail-biting, hair-pulling, and skin-picking). 3P produced greater reductions in craving compared to imaginal retraining alone and wait-list control. Moderation analyses showed a treatment by craving interaction effect, such that participants with high baseline craving ratings benefitted most from the 3P intervention, but this may partly an effect or regression to the mean artifact. Other baseline characteristics, such as age, gender, and alcohol use problem severity did not moderate the effect of treatment on changes in craving. Future research with verified alcohol use disorder and objective measures of changes in drinking are needed to understand the efficacy of this technique for alcohol use disorder treatment.
For policy makers: Although effective alcohol use interventions are available, relapse rates remain high. As treatment seeking and engagement in treatment are relatively low, researchers have called for new, appealing interventions that are brief and convenient. Craving alcohol is a core symptom of alcohol use disorder and an important target for treatment. A new behavioral intervention technique showed immediate reductions in alcohol craving. Future research is needed to understand if this technique actually translates to reduced drinking, how long any observed therapeutic effect may last, and how it could be incorporated into treatment for alcohol or other drug use disorders.
Craving alcohol is a core symptom of alcohol use disorder and an important target for treatment. Although there are many useful psychological and pharmacological interventions, relapse rates remain high. As treatment seeking and engagement in treatment are relatively low, researchers have called for appealing strategies that are convenient and accessible.
A relatively new line of treatment for alcohol use disorder aims at overriding the urge to consume alcohol by changing implicit cognitions through a technique called “approach bias modification.” Implicit cognitions can be described as influences occurring outside one’s conscious awareness such as knowledge, perception, or memory, that influence a person’s behavior.
Implicit cognitions are one potential explanation behind why a person with alcohol use disorder may have the inability to resist the urge to drink. Though initial alcohol or other drug taking may be a fully conscious choice, recent studies have shown that automatic processes play a large role in the development of addiction and the high risk of relapse. That is, there is evidence that drug cues (i.e., reminders in the environment, such as a cocktail glass or the smell of an alcoholic drink) capture automatic attention, evoke activation in the midbrain’s dopamine reward system and engender automatic approach responses making it more likely someone would consume alcohol among individuals with an alcohol or other drug use disorder, each of which may take place largely outside of conscious awareness. These automatically activated processes have been associated with increased alcohol or other drug consumption, despite the fact that individuals may express an explicit wish to quit.
Implicit approach or avoidance reactions are not limited to alcohol or other drug use among individuals who drink or use drugs. Approach/avoidance tendencies may be general bodily reactions to positive and negative stimuli that all people experience. This has been shown in prior research with positive and negative words, fear of spiders, smiling vs. angry faces among individuals with social anxiety, muted reactions in depressed patients vs. non-depressed controls, and more limited approach bias in patients with anorexia nervosa compared to controls. This research tests approach/avoidance tendencies through computerized training paradigms, where, an individual is asked to push away an image or pull the image towards themselves, using a joy stick or button press, for example, and their reaction time is recorded. Shorter reaction times are considered more automatic whereas longer reaction times are considered more controlled. For example, a person with a fear of spiders had a shorter reaction time when asked to push the picture of a spider away with a joy stick than when asked to pull the picture towards them, compared to individuals without a fear of spiders.
Approach bias modification is one type in a set of procedures in psychology called “cognitive bias modification” that aim to directly change these automatic, unconscious tendencies to behave in a certain way in the presence of a particular cue (in this case, alcohol) through repeated practice of a new behavior while imagining or viewing that particular cue (for example, picturing a drink in your mind or looking at a picture of a drink). These procedures are often used the in the treatment of certain anxiety-related disorders, such as nail-biting, skin-picking or hair pulling, where the participant is to practice several times a day the same bodily motion to begin the target behavior, such as bringing their finger to their mouth to bite their nail, then redirecting their body somewhere else, such as touching their finger to their ear. This is practiced over and over to change the automatic behavior that happens outside the person’s conscious awareness. For drinking, this may look like asking a participant to imagine hurling their favorite alcoholic beverage(s) away from themselves; the throwing motion is performed, but the beverage and the situation are only imagined.
In the current study, the researchers conducted a randomized controlled trial testing a brief approach bias modification-based intervention to reduce alcohol craving among adults seeking to reduce problematic drinking.
HOW WAS THIS STUDY CONDUCTED?
This online randomized controlled experiment examined the efficacy of a brief behavioral treatment technique to reduce alcohol craving among (N = 227) adults seeking to reduce problematic drinking.
Participants were recruited online using a participant pool of German-speaking people who have registered for participation in web-based studies. The only inclusion criterion was participants’ self-reported desire to reduce problematic alcohol consumption. Severity of drinking behavior was assessed with a commonly used measure of alcohol use and problems (the 10-item Alcohol Use Disorders Identification Test [AUDIT]).
Participants were asked to rate their current level of craving for alcohol (primary outcome) on a scale ranging from 0 (not at all) to 100 (extreme) after viewing the same three pictures of alcohol cues. Participants were then randomized to 1 out of 5 conditions. Each participant was shown the same photo of a hand holding a full wine glass. Then were given one of the following instructions:
Wait-list control condition: Look at the photo for some time
Zooming-out condition: Make the photo smaller in your imagination (a standardfeature of approach bias modification procedures)
Imaginal retraining without movement condition: Imagine pouring out the liquid or throwing the glass away without making the actual movement
Imaginal retraining condition with movement: Imagine pouring out the liquid or throwing the glass away while making the actual movement
3P (pull-pause-push) condition: Imagine bringing the glass close to your mouth, stopping just short of your mouth, and then pour out the (imagined) liquid or throw the glass away while making the actual movement
In conditions 2-5, participants were asked to perform the exercise at least 5 times; general instructions were essentially the same. After the intervention, participants were asked whether they had actually executed the task, and had to indicate their current level of craving for alcohol on a scale from 0 to 100.
The analysis compared participants’ changes in craving from pre- to post-assessment across the 5 intervention conditions. The researchers ran the same analyses with all participants and again with only the participants who reported they had performed the exercises as instructed (i.e., a “sensitivity analysis”), which was the case for 91.2% of the sample. Participants adhered to the intervention instructions equally across conditions. Both analyses yielded the same pattern of results. In follow-up analyses, they tested if there were differences in intervention effects for participants with higher craving at baseline or other demographic or clinical characteristics.
Slightly more men than women participated (53.7% vs.46.3%). On average, participants were on average in their mid-50s. Approximately one third (32.6%) of the participants had not finished high school. On a commonly used measure of alcohol use and problems, most participants scored in the hazardous or harmful drinking range; 33% were in the alcohol-dependent range (i.e., moderate to severe DSM 5 alcohol use disorder). Intervention condition groups differed on gender and age, where fewer women in conditions 1 (37.2%) and 3 (28.6%) compared to conditions 2 (50%), 4 (53.5%), and 5 (63%), and participants were slightly older in conditions 3 (average 60 years old) and 5 (average 59 years old), and slightly younger in condition 4 (average 49 years old), compared to conditions 1 and 2 where participants were 52 and 54 years old on average, respectively. Groups did not differ on baseline levels of craving, alcohol use and problem severity, depression symptoms, education, nor work status.
WHAT DID THIS STUDY FIND?
Only the 3P condition lessened craving by approximately 1/3.
Alcohol craving did not change in the wait-list control condition, zooming-out condition, imaginal retraining without movement condition, or the imaginal retraining with movement condition. Only the 3P condition lessened craving (by 35%), which was a medium-sized effect.
Participants in the 3P group with high craving benefited the most from the intervention relative to those participants in conditions 1-3.
Participants with higher craving in the 3P condition showed a stronger decline in craving compared to those in the wait-list control, zooming out, and imaginal retraining without movement conditions. It makes sense that participants with the highest cravings had the greatest decline because it is a natural tendency for an extreme state of being to revert back to the middle or average over time (i.e., regress to the mean). Importantly, age and gender, where some group differences emerged, did not influence the effect of the intervention on craving. And, alcohol use problem severity at baseline did not influence the effect of the intervention on craving.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This randomized controlled experiment showed that an intervention focused on changing implicit cognitions through approach bias modification techniques can reduce self-reported alcohol craving among adults seeking to reduce problematic drinking. Specifically, combining two techniques commonly used in treatments for nail-biting, skin-picking, and hair-pulling, i.e. “imaginal retraining” (imagining the alcoholic drink getting smaller, being poured out, or thrown away from you) and “decoupling” (actually practicing the movement of pouring out the drink or pushing it away from you after bringing the drink close to your mouth) was the only variation of treatment that produced a change in alcohol craving ratings compared to imaginal retraining techniques alone or wait-list control.
The researchers have tested imaginal retraining techniques (without decoupling) before to reduce cravings in several domains including: problematic alcohol use; tobacco smoking; and eating among overweight individuals. In similar randomized controlled experiments, imaginal retraining reduced craving for alcohol and self-reported alcohol use, reduced craving for cigarettes and self-reported cigarette smoking, and reduced craving for high-caloric foods and produced greater weight loss. However, in each of these studies including the current study, outcomes were based on self-report and participants were recruited online. Future research with objective measures, such as blood or urine toxicology test verification to confirm alcohol or other drug use, is needed to confirm that reduced craving actually leads to reduced use after these treatment approaches. Also, it is unclear how long such an effect may last and what optimal “dose” or intensity may be needed; it may be that the effect is short-lived and it may need repeating. Different intensities and durations may be needed for different individuals across time. More study is needed in these regards with this specific approach and how it may compare to other similar methods.
Other approach bias modification techniques also show promising outcomes for adults with alcohol use disorder. One study tested an approach bias modification technique using a joystick where you push an image of a drink away from you. Participants completed 4 sessions of the technique before entering inpatient treatment for alcohol use disorder and showed immediate changes in reactivity towards alcohol cues. Those who completed 4 sessions of the technique also had better treatment outcomes one year later. In another study from the same researchers, participants in inpatient treatment for alcohol use disorder showed that reduced craving after completing a similar bias modification technique was associated with reduced activation in the amygdala.
A compelling component of the current intervention is how quick, simple, and easy it would be to implement, especially compared to other bias modification techniques using additional technical equipment, like joy sticks for example. All a person would need is to find a quiet space to imagine the drink (or other subject of craving) and perform the movement (bring the imagined drink up to your mouth and throw it away from you). Given that so few people experiencing alcohol problems access formal care, brief and easy to implement skills like the intervention tested here are so valuable in that they provide more real-time strategies to cope with cravings.
This randomized controlled study provides a jumping off point for further research developing new, brief, and easy to implement treatments for alcohol and other drug use disorders. Future research would need to test the efficacy of this intervention over time, and as well as understand if and how this could be incorporated into various substance use treatment settings. As noted above, for example, how long does this technique reduce cravings? Does craving reduction produced by this technique translate to actual reduced drinking? Who, in particular, is more or less likely to respond? Who would deliver this intervention and in what settings? Could it be used as a self-help mobile app? More research in this line of work is needed to understand how using a technique like this in real-life could reduce craving, and potentially subsequently reduce alcohol use and related harms. If found to be effective, a simple intervention like this could potentially be easily adopted by a large number of people seeking to reduce alcohol craving.
Participants were recruited online by self-reported desire to reduce problematic drinking, and there was no assessment of alcohol use disorder. Future research should verify participants meet criteria for alcohol use disorder to confirm the intervention produces the same effects in a treatment target population.
Since the experimental research was performed exclusively online, it is difficult to know how generalizable the results are to a real-world setting. The researchers simply asked participants if they performed the technique, where participants could simply respond ‘Yes’ or ‘No’ on the survey, with no other way to determine if participants actually did, in fact, perform the technique. This doesn’t provide the researchers an objective, reliable way to determine how faithfully participants adhered to the intended intervention protocol or if they completed it at all. Future research should include more rigorous evaluations of this bias modification skill (e.g., video of participants performing the throwing motion), to have a more accurate understanding of how this could affect craving, especially in naturalistic settings.
BOTTOM LINE
This study found that among 227 adults seeking to reduce problematic alcohol use recruited online in Germany that a new behavioral treatment technique grounded in cognitive bias modification reduced immediate subjective cravings for alcohol by 1/3 compared to active control. Though more research examining this particular approach with more rigorous designs and in different samples can help determine its ultimate utility, cognitive bias modification interventions seem a promising new area for further exploration in the treatment of alcohol and other drug use disorders.
For individuals and families seeking recovery: Implicit cognition is a possible explanation for a common experience described by some people with alcohol use disorder where they have lost the ability to resist the urge to drink – drinking becomes automatic. This new, brief, and convenient behavioral treatment technique aims to change implicit cognitions by having the person imagine hurling their favorite alcoholic beverage(s) away from themselves – the movement is actually performed, but the beverage and the situation are only imagined – and showed immediate reductions in craving after performing the technique. Future research is needed to understand how long such an effect may last and if this actually translates to reduced drinking, and how it could be incorporated into treatment.
For treatment professionals and treatment systems: Although effective alcohol use interventions are available, relapse rates remain high. Approach bias modification techniques used to treat nail-biting, hair-pulling, and skin-picking are new area for exploration in the treatment of addictive behaviors. Imaginal retraining and decoupling when combined showed immediate reductions in alcohol craving. Future research is needed to understand if this technique actually translates to reduced drinking, how long any therapeutic effects may last, for whom in particular it may be helpful or unhelpful, and how it could be incorporated into treatment for alcohol or other drug use disorders.
For scientists:This randomized controlled experiment conducted online with (N = 227) German-speaking adults with a self-reported desire to reduce problematic alcohol consumption showed that a new approach bias modification technique called 3P (pull-pause-push) reduced immediate subjective ratings of alcohol craving compared to active control. 3P combines imaginal retraining and decoupling, a similar approach to treating body-focused repetitive behaviors (e.g., nail-biting, hair-pulling, and skin-picking). 3P produced greater reductions in craving compared to imaginal retraining alone and wait-list control. Moderation analyses showed a treatment by craving interaction effect, such that participants with high baseline craving ratings benefitted most from the 3P intervention, but this may partly an effect or regression to the mean artifact. Other baseline characteristics, such as age, gender, and alcohol use problem severity did not moderate the effect of treatment on changes in craving. Future research with verified alcohol use disorder and objective measures of changes in drinking are needed to understand the efficacy of this technique for alcohol use disorder treatment.
For policy makers: Although effective alcohol use interventions are available, relapse rates remain high. As treatment seeking and engagement in treatment are relatively low, researchers have called for new, appealing interventions that are brief and convenient. Craving alcohol is a core symptom of alcohol use disorder and an important target for treatment. A new behavioral intervention technique showed immediate reductions in alcohol craving. Future research is needed to understand if this technique actually translates to reduced drinking, how long any observed therapeutic effect may last, and how it could be incorporated into treatment for alcohol or other drug use disorders.