
How important are therapists in addiction treatment? Contrasting web-based and clinician delivered cognitive behavioral therapy (CBT) for substance use disorder
Limited access to evidence-based, clinician-delivered interventions for substance use disorder has given rise to a number of web-based interventions, which may potentially provide greater accessibility to treatment in addition to cost savings for healthcare systems. While a growing body of evidence suggests web-based interventions may be effective, this study was the first to test web-based cognitive behavioral therapy (CBT) and gold-standard clinician delivered CBT in the same trial.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Individuals seeking recovery from substance use disorder are often confronted by significant barriers that prevent them from receiving evidence-based treatment such as insufficient health insurance, difficulty physically getting to appointments, or insufficient motivation to overcome these, as well as numerous other barriers to treatment. Web-based interventions have the potential to surmount such barriers because they can be delivered at very low cost and can be accessed from home or just about anywhere. This study asked if a high quality, automated, online CBT treatment program called CBT4CBT—developed by researchers at Yale University—could do as well as gold-standard, clinician-delivered CBT for substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
DESIGN: This was a randomized controlled trial in which 137 individuals who met Diagnostic and Statistical Manual of Mental Disorders-IV-TR criteria for current substance abuse or dependence were randomly assigned to receive treatment as usual (i.e., standard care provided by the study recruitment site), 12 weeks of weekly individual CBT, or 12 weeks of weekly CBT4CBT with brief weekly clinician check-ins.
- READ MORE ON STUDY METHODS
-
Participants were randomly assigned using the urn randomization technique, which attempts to match the treatment groups on individual factors such as gender, ethnicity, education level, primary substance used (i.e., cocaine, marijuana, other), self-reported familiarity with computers, and referral through the criminal justice system. This kind of randomization helps reduce the likelihood that study results will be influenced by individual participant factors differing between groups.
Participants randomized to the treatment as usual group were offered standard treatment at the clinic, which consisted of weekly group, and/or individual therapy, as determined by the clinical team. Treatment as usual varied, but could include such topics as motivational interviewing, life skills, relapse prevention, harm reduction, mindfulness, women and trauma, health and recovery, and Latino recovery.
Participants randomized to the clinician-delivered CBT group received 12, weekly individual sessions of manual guided CBT that covered functional analysis of thoughts, feelings and behaviors, coping skills training, practice exercises, explanation of CBT concepts, and CBT homework.
Participants randomized to receive web-based CBT (CBT4CBT) received 12, weekly online CBT session sessions plus weekly 10-minute, in-person monitoring sessions intended to evaluate participants’ current functional status and safety and to review their use of the CBT4CBT program. The 12-week CBT4CBT course contains seven core CBT skill topics (modules) that include on-screen narration, graphic animation, quizzes, and other interactive exercises to teach and model effective use of skills. Each module presents videos demonstrating use of a targeted CBT skill and concludes with printable take-home practice exercises (homework).
SETTING: The Substance Use Treatment Unit of the Connecticut Mental Health Center in New Haven, CT.
PARTICIPANTS: Participants were recruited from the Substance Use Treatment Unit of the Connecticut Mental Health Center in New Haven between January 2012 and October 2016. To be eligible for the study, individuals needed to be adults meeting Diagnostic and Statistical Manual of Mental Disorders-IV-TR criteria for current (i.e., past 30 days) cocaine, marijuana, opioid, or alcohol abuse or dependence. 191 individuals were screened for participation, and 137 were eligible for the study.
MEASUREMENT: Participants were assessed before treatment, weekly during treatment, at the 12-week treatment termination point, and 1, 3, and 6 months after the treatment termination. Self–reports of drug use were verified through urine toxicology screens, for which samples were obtained at every assessment visit. Breath alcohol samples were also collected at each visit.
 WHAT DID THIS STUDY FIND?
WHAT DID THIS STUDY FIND?
Contrary to the expectations of the authors, treatment retention was significantly higher among those receiving the web-based CBT4CBT intervention (a mean of 62 out of 84 days completed), lowest in the clinician-delivered CBT condition (43 days), and intermediate in the treatment-as-usual condition (55 days).
The authors did an intent-to-treat analysis to determine which intervention performed best (meaning they included all participants that were initially randomly assigned to one of the three intervention conditions in their analysis, not just those that completed treatment. Analysis of the data collected during the active treatment phase of the study indicated reductions in the frequency of any substance use for the whole sample, meaning on average participants saw reductions in substance use regardless of the treatment group they were randomized to (Figure 1).

Figure 1. Change in frequency of any drug or alcohol use during the 12-week treatment phase of the study. Groups were similar in terms of frequency of any drug or alcohol use at baseline (week 0) but had different trajectories of frequency of any drug or alcohol use reduction showing both web-based cognitive-behavioral therapy (CBT4CBT) and clinician-delivered CBT outperformed treatment as usual.
Also, during the treatment phase of the study, the authors observed greater reductions in frequency of any drug or alcohol use for clinician-delivered CBT compared with treatment as usual, and for CBT4CBT compared with treatment as usual (Figure 1). Notably, these findings were similar regardless of sample examined (e.g., all participants assigned to treatment including data after dropout, treatment initiators, treatment exposed, or excluding participants whose primary substance was not marijuana, cocaine, or alcohol). Both clinician-delivered, and web-based CBT outperformed treatment as usual during the 12-week treatment phase of the study.
Over the follow-up period, web-based CBT significantly outperformed treatment as usual indicating sustained effects over time for the CBT4CBT intervention relative to treatment as usual (Figure 2). Clinician-delivered CBT, however, did not perform significantly better than treatment as usual over the follow-up period.
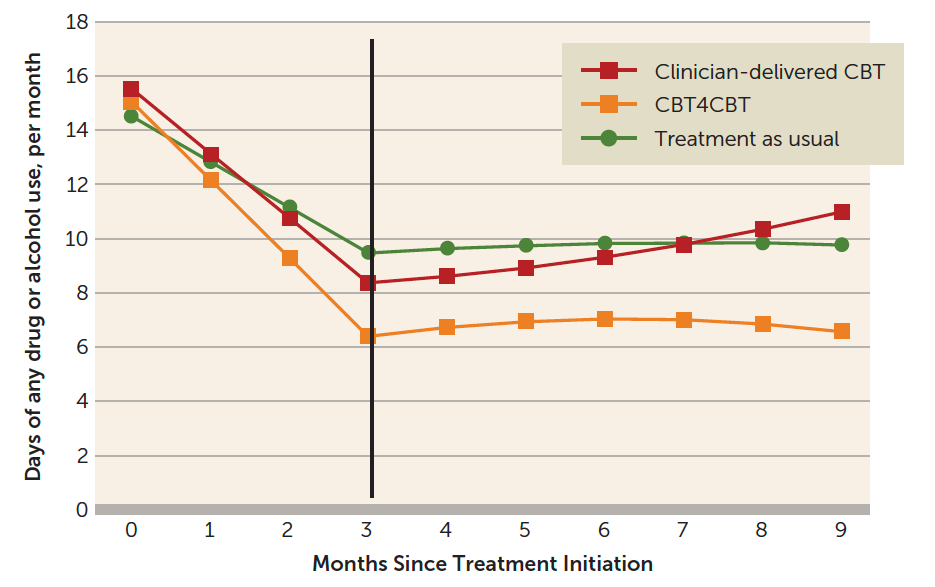
Figure 2. Frequency of any drug or alcohol use over the 6-month follow-up phase of the study. Web-based cognitive-behavioral therapy (CBT4CBT) outperformed treatment as usual, but clinician-delivered CBT did not.
Notably, the percentage of drug-free urine specimens was highest in the CBT4CBT plus monitoring group (37%), lowest (i.e., worse) in the clinician-delivered CBT group (33.1%), and intermediate in the treatment-as-usual group (34.3%), but these differences were not statistically significant. Rates of individuals no longer meeting Diagnostic and Statistical Manual of Mental Disorders IV-TR diagnostic threshold for current substance dependence at treatment termination also favored CBT4CBT plus monitoring (66.7%) over clinician-delivered CBT(51.6%) and treatment as usual (42.9%), which also fell short of statistical significance.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Findings support the safety, feasibility, and utility of the CBT4CBT web-based CBT intervention provided with minimal clinical monitoring. During the treatment phase of the study, both CBT4CBT, and clinician-delivered CBT outperformed treatment as usual. Over the follow-up period, CBT4CBT performed better than treatment as usual in terms of number of days of alcohol and drug use, whereas clinician-delivered CBT was statistically equivalent to treatment as usual. Those randomized to CBT4CBT showed the greatest increase in knowledge of CBT concepts. This computerized version of CBT thus appears to be an engaging and useful approach for the treatment of substance use disorder.
Although those assigned to clinician-delivered CBT did show greater reductions in substance use during the treatment phase compared with those assigned to treatment as usual, the clinician-delivered CBT group also had the poorest level of treatment retention, and the lowest rates of abstinence during the follow-up period. Despite well-trained clinicians delivering high-quality treatment, participants assigned to clinician-delivered CBT dropped out of treatment sooner, had a greater number of withdrawals from treatment, and had the lowest rates of follow-up data collected. It may be that weekly one-on-one CBT was too demanding for patients sampled in the study, many of whom were referred to treatment by the criminal justice system, and who may have had less motivation to receive substance use disorder care than those self-referring to care. It is also possible that individuals coming to the study through the criminal justice system have less resources at their disposal to support addiction recovery (e.g., financial means, social support, stable housing). It is noteworthy too that the CBT4CBT group had a smaller number of participants referred through the criminal justice system compared to traditional CBT and treatment as usual groups (CBT4CBT 23.7%; traditional CBT 34.7%; treatment as usual 44%), which may in part some of these observed differences. The authors did not have a sample size sufficient to test statistically whether criminal justice system involvement influenced study outcomes.
Interestingly, the lack of a therapist while delivering CBT may evoke less resistance among those who are perhaps more ambivalent about change making the web-based version perhaps more effective. The patient is left to ponder themselves without what may construed as “an agenda” by a therapist for those on the fence about changing their substance use. More research is needed to understand the exact mechanisms for these different than expected outcomes.
Findings from this study comparing clinician-delivered and web-based CBT to treatment as usual, speak to the promise of interventions such as CBT4CBT, more research is needed, however, before concrete conclusions can be made about its effectiveness. These first pass results, nevertheless, show great promise, and speak to the potential of web-based treatments such as CBT4CBT, as well as other online addiction interventions like Therapeutic Education System (www.sudtech.org/about) to reach a lot more people suffering from substance-related problems.
- LIMITATIONS
-
- The present study makes an important contribution to the scientific literature on web-based addictions interventions. It did not, however, compare web-based CBT to another empirically-supported approaches like Motivational Enhancement Therapy or Twelve-Step Facilitation. More studies are needed to begin to determine web-based CBT’s effectiveness in comparison to other evidence-based addiction treatments.
- Participants receiving CBT4CBT had weekly check-ins with study stuff, which typically would not be part of this treatment. This may limit how well the authors’ findings generalize to the real world.
- Though not necessarily a limitation per se, but important to bear in mind, 35% of study participants were mandated to treatment by the criminal justice system and these differed substantially between groups after randomization. These individuals may have been less motivated to be in treatment (compared to individuals seeking treatment of their own volition) and thus greater affinity for the web-based intervention because of the flexibility it provides. The sample size of this study limited the authors’ ability to make substance use outcome comparisons between participants mandated to treatment, and those attending treatment voluntarily.
- Patients in this study were treated with an array of medications, which could have influenced results, although groups were not significantly different in terms of medications.
BOTTOM LINE
- For individuals & families seeking recovery: The web-based CBT program CBT4CBT may have the potential to work as a stand-alone treatment for substance use disorder, and it may also be helpful as an add-on to usual clinical care. It is important to note that the study reviewed here tested a specific web-based CBT platform. The authors’ findings may not generalize to other web-based CBT programs, which are likely to vary in quality.
- For scientists: Web-based CBT platforms are increasingly demonstrating their potential to provide care for patients with limited access to treatment. Though CBT4CBT outperformed clinician-delivered CBT on a number of measures in this study, more research is needed to establish its effectiveness and who, in particular, may or may not benefit. For instance, the present study included many individuals who were mandated to treatment by the criminal justice system. This study should be replicated in different samples. Further, to increase the ecological validity of findings, future studies should deliver CBT4CBT without weekly clinician check-ins. Future studies should also compare CBT4CBT to other empirically supported treatments such as Motivational Enhancement Therapy or Twelve-Step Facilitation.
- For policy makers: Web-based CBT programs have tremendous potential to increase access to evidence-based care, and can be delivered at a fraction of the price of clinic-based care. Increasing access to these interventions could have tremendous public health benefit.
- For treatment professionals and treatment systems: A growing base of evidence supports the efficacy of the CBT4CBT web-based intervention. Given its accessibility and cost-effectiveness, CBT4CBT should be considered as a potential add-on to reinforce clinic-based treatment, or for individuals without access to clinic-based care, it should be considered as a first-line treatment
CITATIONS
Kiluk, B. D., Nich, C., Buck, M. B., Devore, K. A., Frankforter, T. L., LaPaglia, D. M., … & Carroll, K. M. (2018). Randomized clinical trial of computerized and clinician-delivered CBT in comparison with standard outpatient treatment for substance use disorders: primary within-treatment and follow-up outcomes. American Journal of Psychiatry, 175(9), 853-863.