Investigating sub-types of alcohol use disorder to improve treatment response
Each year, over 3 million deaths result from harmful use of alcohol in the United States and around the world. While many good treatments exist, there have been efforts to further boost treatment response through “precision medicine” approaches designed to find better matches between patient subtypes and corresponding types of treatment. This study sought to uncover more valid and clinically useful subtypes of alcohol use disorder in order to enhance the effectiveness of treatment.
Alcohol is responsible for 140,000 deaths annually in the US. Finding more effective treatments for alcohol use disorder has remained a top clinical and public health priority. For almost 100 years there have been documented clinical and public health efforts to identify different “subtypes” of “alcoholics” and other addicted persons to try to arrive at more precise treatment matches for more specific sub-groups and thus more effective treatments. Many clinicians and researchers have provided various typologies based on careful clinical observation or data-driven statistical modeling approaches. See work by Silkworth, Jelllinek, Cloninger, Babor, Hesselbrock, and Moss as stand-out examples. Such groupings have produced some interesting and compelling typologies, but these have failed to deliver on the promise of identifying robust and clinically meaningful subtypes that can lead to enhancements in “precision medicine”.
Alcohol use disorder is classified currently as a single dimensional disorder with mild, moderate, and severe subclassifications based solely on a simple sum of the number of symptoms met from a total of 11 possible symptoms. These simplified quantitatively-based subclassifications, however, may miss important qualitative differences in the impact of alcohol use disorder and how best to treat it. Similar to other attempts over the years, this study analyzed the most recent DSM-5 alcohol use disorder criteria classification to see whether certain types of symptoms naturally seem to cluster together in the hope of uncovering more meaningful diagnostic sub-groupings than merely “mild”, “moderate”, and “severe” based only a simple sum of any of 11 symptoms. The ability to identify more meaningful and similar sub-groups of individuals with the disorder may help improve treatment response by tailoring and matching treatments to these different sub-groups’ needs – often referred to as “precision medicine”.
Identifying more meaningful typologies of alcohol use disorder than ones merely based on simple sums of symptoms might be especially relevant for young adults. Young adults aged 18 to 25 tend to have the highest prevalence of past 30-day binge and heavy alcohol use as well as alcohol use disorder compared to any other age-group across the life course. In 2020, 31.4% reported binge drinking and 8.6% reported heavy alcohol use compared to 22.9% and 6.7% respectively among adults 26 and older. Given these high rates of harmful/hazardous use and alcohol use disorder, this age-range is a useful one in which to study these phenomena. Identifying, for example, who might be at greater risk for persisting alcohol use disorder versus have a subtype that may be more context-specific (e.g., due to being in a heavy drinking environment, such as college) based on an actual experiential clustering of certain symptoms, could help tailor and better match interventions to these specific sub-groups’ needs. The present study sought to investigate alcohol use disorder typologies in young adults and examine the unique protective and risk factors associated with different typologies.
HOW WAS THIS STUDY CONDUCTED?
This cross-sectional study used a convenience sample of 1,390 young adults (18-30 years old). Participants were recruited through flyers, business cards posted in the community, and posting on the Indiana University classifieds webpage. A wide variety of alcohol problems, from no problems to severe problems, were sought. Individuals were excluded if they had an externalizing disorder, which are characterized by maladaptive behaviors directed toward an individual’s environment (e.g., conduct disorder), without the presence of alcohol use disorder. Participants could, however, have alcohol use disorder in addition to another externalizing disorder. All participants completed a collection of measures to determine DSM-5 alcohol use disorder diagnosis (along with other substance use disorders), alcohol use disorder symptoms, acute alcohol use problems, treatment seeking, alcohol and other substance use, conduct disorder symptoms, anxiety, depression, borderline personality disorder, experience seeking, and impulsivity. The study used a statistical technique called latent class analysis to identify if there were naturally occurring clusters of alcohol use disorder symptoms and then investigated if these clusters were associated with individual characteristics (experience seeking, anxiety, etc.).
The final sample of 1,390 young adults included an over-representation of alcohol problems with 65% meeting DSM-5 criteria for alcohol use disorder. Additionally, 40% of the sample meet criteria for cannabis use disorder and 18% meet criteria for another substance use disorder. Participants’ age ranged from 18 to 30 years old and were 21 years old, on average. The sample was 48% female and 78% White.
WHAT DID THIS STUDY FIND?
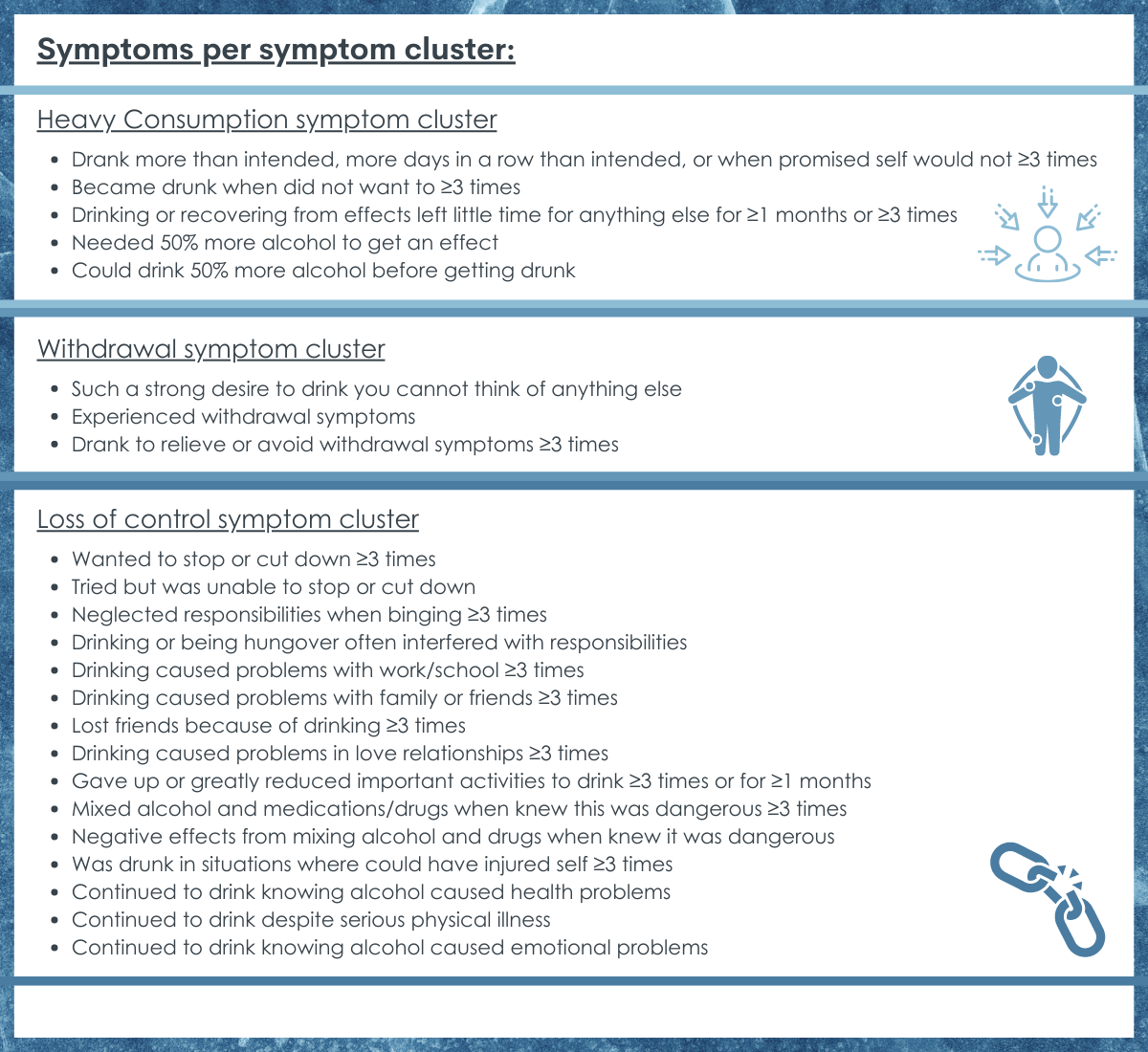
Four symptom clusters indicated a general continuum of severity, yet were qualitatively different.
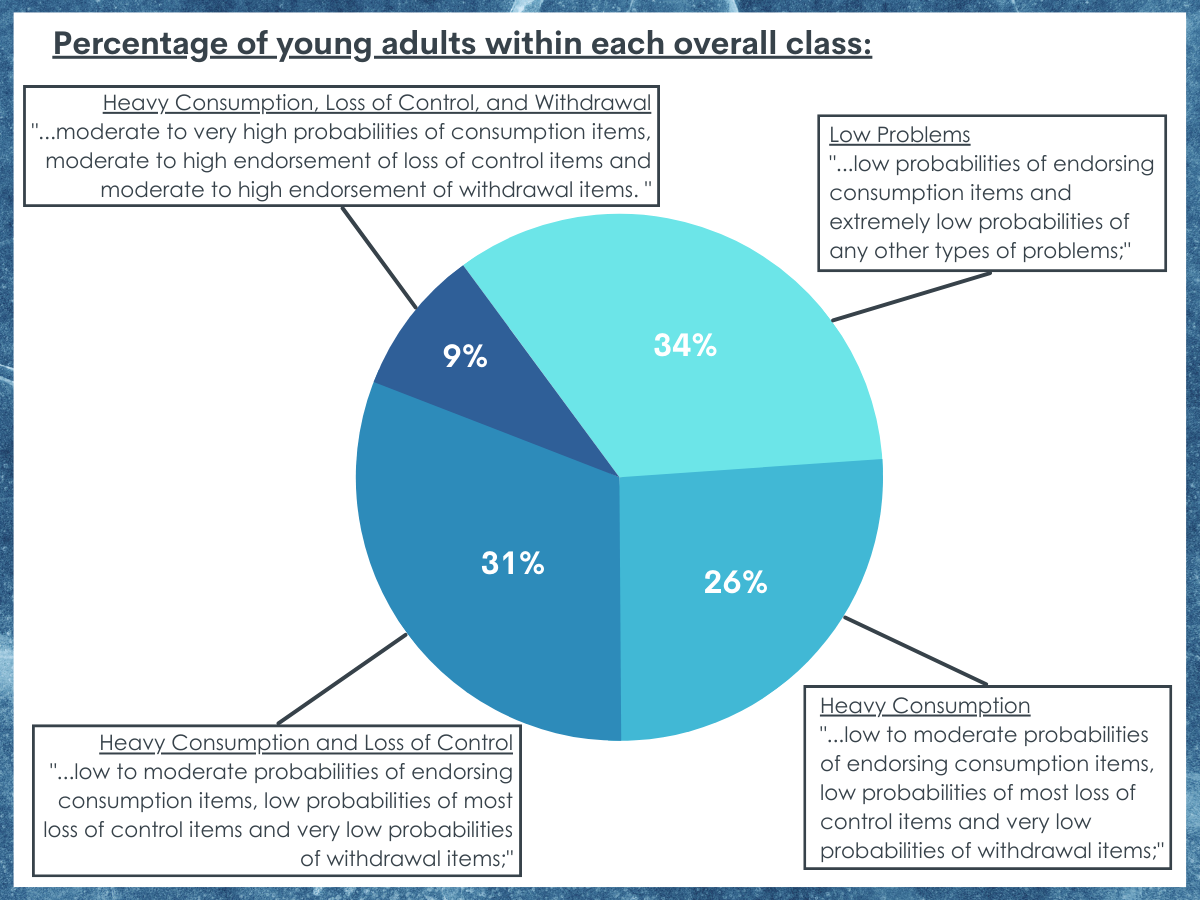
Analysis of alcohol use disorder symptoms revealed four theoretically and empirically supported clusters. These were labeled as: ‘Low Problems’, ‘Heavy Consumption’, ‘Consumption and Loss of Control’, and ‘Consumption, Loss of Control, and Withdrawal’. The classes represented 34%, 26%, 31%, and 9% of the sample respectively. The results showed an additive pattern of increasing severity. However, this pattern was not linear. Each of the classes represented a qualitatively different cluster of symptoms.
Individuals in the ‘Heavy Consumption’ group were more likely to report more frequent, higher quantities, and more binge days of alcohol use compared to those in the ‘Low Problems’ grouping. However, alcohol use did not vary between the two highest severity groups – ‘Consumption and Loss of Control’ and ‘Consumption, Loss of Control, and Withdrawal’. Those in the ‘Heavy Consumption’ group were more likely to exhibit the experience-seeking trait. There was little to no difference in the occurrence of depression between the groups, but anxiety was more likely in the two highest severity groups. Substance use other than alcohol increased in a linear fashion such that individuals in each subsequent severity group were more likely to report additional substance use. Similarly, impulsivity, conduct problems, and borderline personality traits all were more likely to be endorsed in subsequent severity groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Overall, this study of 1,390 young adults found that alcohol use disorder symptoms tended to cluster together into three groups. These findings partially support the conceptualization of alcohol use disorder as it appears in the DSM-5. The clusters did represent increasing severity: ‘Low Problems’, ‘Heavy Consumption’, ‘Consumption and Loss of Control’, and ‘Consumption, Loss of Control, and Withdrawal’. However, each cluster had a unique symptom profile as represented by the cluster name, such that each sequential group added a new cluster of symptoms (e.g., heavy consumption then loss of control then withdrawal). Individuals in the ‘Low Problems’ group reported fewer drinks, less frequent drinking, and less binge drinking as well other risks and difficulties (e.g., other drug use, impulsivity, conduct symptoms, depression) compared to the other groups. The ‘Heavy Consumption’ group reported more problems and alcohol use compared to the ‘Low Problem’ group, but fewer and less frequent drinks and problems compared to the other two groups. The amount and frequency of alcohol use, however, did not differ between the two later groups. Conversely, the ‘Consumption, Loss of Control, and Withdrawal’ group reported more difficulties and risks (e.g., acute alcohol problems, drug use, conduct symptoms, impulsivity, anxiety, and borderline personality traits) compared to all other groups. The higher likelihood of impairment in this group suggests that those individuals might require the most acute and extensive support services compared to the other groups. This study suggests that conceptualizing alcohol use disorder symptoms as having three subscales measuring consumption, loss of control, and withdrawal might possibly be more useful for developing interventions, treatment, and policy.
The existing formulation of alcohol use disorder requires endorsement of any 2 symptom criteria. However, this study shows that which symptoms an individual endorses might be useful in determining alcohol use disorder severity.
For example, alcohol consumption appears to be useful in identifying those with and without alcohol use-related problems, yet it does not distinguish between the two groups with the highest severity. This pattern is consistent with other research showing that consumption symptoms have lower predictive power compared to other symptoms. Conversely, the endorsement of symptoms related to withdrawal almost exclusively appeared in the most severe group. Identifying which group an individual most closely resides in might aid treatment planning. For example, those in the ‘Heavy Consumption’ group are less impaired, yet they are more likely to endorse the experience-seeking trait. Those in this group might benefit most from education and harm reduction strategies. On the other hand, those in the highest severity group might require physiological stabilization (e.g., medications to manage withdrawal) prior to other forms of treatment.
These findings suggest that the variation among individuals diagnosed with alcohol use disorder might be conceptualized as including three subtypes related to consumption, loss of control, and withdrawal. This conceptualization, although representative of increasing severity like alcohol use disorder’s current diagnostic system, may be more useful in treatment planning and policy making compared to the existing mild, moderate, and severe subclassifications that appear in the DSM-5 that is based merely on a sum total of the number of symptoms met. These typologies of alcohol use disorder may be especially relevant for treatment planning and policy for young adults, who have disproportionally higher rates of alcohol use disorder and alcohol-related harms compared to young and older age groups.
Unknown from this study is whether such subtypes represent robust and stable patterns of alcohol use and symptoms in these individuals or whether at least some may be phases or levels of severity, problems, and impairment, that may get worse or better or otherwise morph over time – at least for some.
These data were collected from young adults 18-30 years old (average = 21.43) who mostly identified as White (78%), the findings may not generalize to individuals who are older, younger, or with different demographic characteristics.
Although the 4-class solution was the most parsimonious and theoretically meaningful solution, the analysis found a better fit with 5- and 6-class models. Although the 5- and 6-class models comprised very few individuals, a larger and more diverse sample may support additional typologies not used in this study.
BOTTOM LINE
In this study of young adults with a high prevalence of alcohol-related problems, the researchers found that individuals could be meaningfully grouped in clusters representing qualitatively different symptom groupings with increasing severity: ‘Low Problems’, ‘Heavy Consumption’, ‘Consumption and Loss of Control’, and ‘Consumption, Loss of Control, and Withdrawal’. The simple summing of any endorsed symptoms in DSM-5 to create levels of severity (i.e., “mild” “moderate” “severe”) may not actually be that useful in identifying clinically meaningful groups or typologies of individuals with alcohol use disorder. Clinicians and treatment providers would likely benefit from knowing not only if an individual is diagnosed with an alcohol use disorder but also what is the nature and impact of that disorder. Unclear from this research is how robust and stable these subtypes are and whether these do in fact represent “types” or in some cases, “phases”, of alcohol use disorder whereby alcohol-related symptoms and impairment and negative impacts all change over time.
For individuals and families seeking recovery: If you or a loved one is experiencing symptoms related to alcohol-use, it is likely beneficial to seek medical diagnosis and support. Even if you or a loved one may not be experiencing severe impairment, early screening is likely to help link to supports.
For treatment professionals and treatment systems: Although an alcohol use disorder diagnosis may signal the need for important resources (e.g., treatment, recovery supports), like any substance use disorder diagnosis there is extensive variation among individuals in the degree of alcohol involvement, impairment, and symptoms of “alcohol use disorder.” Although the DSM-5 approach to alcohol use disorder diagnosis may be useful to identify young adults with some kind of alcohol use disorder, identifying more specifically what subtype of alcohol use disorder an individual fits would enhance precision medicine and help programs better tailor treatment to meet the needs of specific sub-groups.
For scientists:Receiving an alcohol use disorder diagnosis can be a critical step in facilitating appropriate supports and treatment and limiting future harms. However, the heterogeneity in in alcohol involvement, impairment, and symptoms, among individuals with alcohol use disorder makes establishing more specific clinical guidelines difficult. This study presents a way (latent class analysis) of establishing symptom clusters. Future studies could build upon this study by recruiting a more diverse sample, particularly with more age and racial/ethnic diversity. Similarly, results may also differ across geographic and clinical settings. Cultural norms, expectancies, and supports may alter the presentation of symptoms and typologies. Methodological studies that balance diagnostic sensitivity and specificity seem needed to identify individuals with alcohol use disorder as well as demarcate clinically relevant typologies. Also unknown is how robust these types are as stable phenotypes or represent dynamic phases of the disorder at least for some.
For policy makers: Alcohol use disorder can be a crucial first step to receiving treatment and reducing harm. This study found that although DSM-5 alcohol use disorder diagnostic category requires only 2 symptoms from 11 to be met included in the category its simple summing of endorsed symptoms to arrive at clinically meaningful and medically responsive subtypes may not be the best way to identify the severity of an alcohol use disorder and which approaches to take. More funding to support methodological exploration of the dynamic clinical course of alcohol use disorder could inform clinical care and public health interventions.
Alcohol is responsible for 140,000 deaths annually in the US. Finding more effective treatments for alcohol use disorder has remained a top clinical and public health priority. For almost 100 years there have been documented clinical and public health efforts to identify different “subtypes” of “alcoholics” and other addicted persons to try to arrive at more precise treatment matches for more specific sub-groups and thus more effective treatments. Many clinicians and researchers have provided various typologies based on careful clinical observation or data-driven statistical modeling approaches. See work by Silkworth, Jelllinek, Cloninger, Babor, Hesselbrock, and Moss as stand-out examples. Such groupings have produced some interesting and compelling typologies, but these have failed to deliver on the promise of identifying robust and clinically meaningful subtypes that can lead to enhancements in “precision medicine”.
Alcohol use disorder is classified currently as a single dimensional disorder with mild, moderate, and severe subclassifications based solely on a simple sum of the number of symptoms met from a total of 11 possible symptoms. These simplified quantitatively-based subclassifications, however, may miss important qualitative differences in the impact of alcohol use disorder and how best to treat it. Similar to other attempts over the years, this study analyzed the most recent DSM-5 alcohol use disorder criteria classification to see whether certain types of symptoms naturally seem to cluster together in the hope of uncovering more meaningful diagnostic sub-groupings than merely “mild”, “moderate”, and “severe” based only a simple sum of any of 11 symptoms. The ability to identify more meaningful and similar sub-groups of individuals with the disorder may help improve treatment response by tailoring and matching treatments to these different sub-groups’ needs – often referred to as “precision medicine”.
Identifying more meaningful typologies of alcohol use disorder than ones merely based on simple sums of symptoms might be especially relevant for young adults. Young adults aged 18 to 25 tend to have the highest prevalence of past 30-day binge and heavy alcohol use as well as alcohol use disorder compared to any other age-group across the life course. In 2020, 31.4% reported binge drinking and 8.6% reported heavy alcohol use compared to 22.9% and 6.7% respectively among adults 26 and older. Given these high rates of harmful/hazardous use and alcohol use disorder, this age-range is a useful one in which to study these phenomena. Identifying, for example, who might be at greater risk for persisting alcohol use disorder versus have a subtype that may be more context-specific (e.g., due to being in a heavy drinking environment, such as college) based on an actual experiential clustering of certain symptoms, could help tailor and better match interventions to these specific sub-groups’ needs. The present study sought to investigate alcohol use disorder typologies in young adults and examine the unique protective and risk factors associated with different typologies.
HOW WAS THIS STUDY CONDUCTED?
This cross-sectional study used a convenience sample of 1,390 young adults (18-30 years old). Participants were recruited through flyers, business cards posted in the community, and posting on the Indiana University classifieds webpage. A wide variety of alcohol problems, from no problems to severe problems, were sought. Individuals were excluded if they had an externalizing disorder, which are characterized by maladaptive behaviors directed toward an individual’s environment (e.g., conduct disorder), without the presence of alcohol use disorder. Participants could, however, have alcohol use disorder in addition to another externalizing disorder. All participants completed a collection of measures to determine DSM-5 alcohol use disorder diagnosis (along with other substance use disorders), alcohol use disorder symptoms, acute alcohol use problems, treatment seeking, alcohol and other substance use, conduct disorder symptoms, anxiety, depression, borderline personality disorder, experience seeking, and impulsivity. The study used a statistical technique called latent class analysis to identify if there were naturally occurring clusters of alcohol use disorder symptoms and then investigated if these clusters were associated with individual characteristics (experience seeking, anxiety, etc.).
The final sample of 1,390 young adults included an over-representation of alcohol problems with 65% meeting DSM-5 criteria for alcohol use disorder. Additionally, 40% of the sample meet criteria for cannabis use disorder and 18% meet criteria for another substance use disorder. Participants’ age ranged from 18 to 30 years old and were 21 years old, on average. The sample was 48% female and 78% White.
WHAT DID THIS STUDY FIND?
Four symptom clusters indicated a general continuum of severity, yet were qualitatively different.
Analysis of alcohol use disorder symptoms revealed four theoretically and empirically supported clusters. These were labeled as: ‘Low Problems’, ‘Heavy Consumption’, ‘Consumption and Loss of Control’, and ‘Consumption, Loss of Control, and Withdrawal’. The classes represented 34%, 26%, 31%, and 9% of the sample respectively. The results showed an additive pattern of increasing severity. However, this pattern was not linear. Each of the classes represented a qualitatively different cluster of symptoms.
Individuals in the ‘Heavy Consumption’ group were more likely to report more frequent, higher quantities, and more binge days of alcohol use compared to those in the ‘Low Problems’ grouping. However, alcohol use did not vary between the two highest severity groups – ‘Consumption and Loss of Control’ and ‘Consumption, Loss of Control, and Withdrawal’. Those in the ‘Heavy Consumption’ group were more likely to exhibit the experience-seeking trait. There was little to no difference in the occurrence of depression between the groups, but anxiety was more likely in the two highest severity groups. Substance use other than alcohol increased in a linear fashion such that individuals in each subsequent severity group were more likely to report additional substance use. Similarly, impulsivity, conduct problems, and borderline personality traits all were more likely to be endorsed in subsequent severity groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Overall, this study of 1,390 young adults found that alcohol use disorder symptoms tended to cluster together into three groups. These findings partially support the conceptualization of alcohol use disorder as it appears in the DSM-5. The clusters did represent increasing severity: ‘Low Problems’, ‘Heavy Consumption’, ‘Consumption and Loss of Control’, and ‘Consumption, Loss of Control, and Withdrawal’. However, each cluster had a unique symptom profile as represented by the cluster name, such that each sequential group added a new cluster of symptoms (e.g., heavy consumption then loss of control then withdrawal). Individuals in the ‘Low Problems’ group reported fewer drinks, less frequent drinking, and less binge drinking as well other risks and difficulties (e.g., other drug use, impulsivity, conduct symptoms, depression) compared to the other groups. The ‘Heavy Consumption’ group reported more problems and alcohol use compared to the ‘Low Problem’ group, but fewer and less frequent drinks and problems compared to the other two groups. The amount and frequency of alcohol use, however, did not differ between the two later groups. Conversely, the ‘Consumption, Loss of Control, and Withdrawal’ group reported more difficulties and risks (e.g., acute alcohol problems, drug use, conduct symptoms, impulsivity, anxiety, and borderline personality traits) compared to all other groups. The higher likelihood of impairment in this group suggests that those individuals might require the most acute and extensive support services compared to the other groups. This study suggests that conceptualizing alcohol use disorder symptoms as having three subscales measuring consumption, loss of control, and withdrawal might possibly be more useful for developing interventions, treatment, and policy.
The existing formulation of alcohol use disorder requires endorsement of any 2 symptom criteria. However, this study shows that which symptoms an individual endorses might be useful in determining alcohol use disorder severity.
For example, alcohol consumption appears to be useful in identifying those with and without alcohol use-related problems, yet it does not distinguish between the two groups with the highest severity. This pattern is consistent with other research showing that consumption symptoms have lower predictive power compared to other symptoms. Conversely, the endorsement of symptoms related to withdrawal almost exclusively appeared in the most severe group. Identifying which group an individual most closely resides in might aid treatment planning. For example, those in the ‘Heavy Consumption’ group are less impaired, yet they are more likely to endorse the experience-seeking trait. Those in this group might benefit most from education and harm reduction strategies. On the other hand, those in the highest severity group might require physiological stabilization (e.g., medications to manage withdrawal) prior to other forms of treatment.
These findings suggest that the variation among individuals diagnosed with alcohol use disorder might be conceptualized as including three subtypes related to consumption, loss of control, and withdrawal. This conceptualization, although representative of increasing severity like alcohol use disorder’s current diagnostic system, may be more useful in treatment planning and policy making compared to the existing mild, moderate, and severe subclassifications that appear in the DSM-5 that is based merely on a sum total of the number of symptoms met. These typologies of alcohol use disorder may be especially relevant for treatment planning and policy for young adults, who have disproportionally higher rates of alcohol use disorder and alcohol-related harms compared to young and older age groups.
Unknown from this study is whether such subtypes represent robust and stable patterns of alcohol use and symptoms in these individuals or whether at least some may be phases or levels of severity, problems, and impairment, that may get worse or better or otherwise morph over time – at least for some.
These data were collected from young adults 18-30 years old (average = 21.43) who mostly identified as White (78%), the findings may not generalize to individuals who are older, younger, or with different demographic characteristics.
Although the 4-class solution was the most parsimonious and theoretically meaningful solution, the analysis found a better fit with 5- and 6-class models. Although the 5- and 6-class models comprised very few individuals, a larger and more diverse sample may support additional typologies not used in this study.
BOTTOM LINE
In this study of young adults with a high prevalence of alcohol-related problems, the researchers found that individuals could be meaningfully grouped in clusters representing qualitatively different symptom groupings with increasing severity: ‘Low Problems’, ‘Heavy Consumption’, ‘Consumption and Loss of Control’, and ‘Consumption, Loss of Control, and Withdrawal’. The simple summing of any endorsed symptoms in DSM-5 to create levels of severity (i.e., “mild” “moderate” “severe”) may not actually be that useful in identifying clinically meaningful groups or typologies of individuals with alcohol use disorder. Clinicians and treatment providers would likely benefit from knowing not only if an individual is diagnosed with an alcohol use disorder but also what is the nature and impact of that disorder. Unclear from this research is how robust and stable these subtypes are and whether these do in fact represent “types” or in some cases, “phases”, of alcohol use disorder whereby alcohol-related symptoms and impairment and negative impacts all change over time.
For individuals and families seeking recovery: If you or a loved one is experiencing symptoms related to alcohol-use, it is likely beneficial to seek medical diagnosis and support. Even if you or a loved one may not be experiencing severe impairment, early screening is likely to help link to supports.
For treatment professionals and treatment systems: Although an alcohol use disorder diagnosis may signal the need for important resources (e.g., treatment, recovery supports), like any substance use disorder diagnosis there is extensive variation among individuals in the degree of alcohol involvement, impairment, and symptoms of “alcohol use disorder.” Although the DSM-5 approach to alcohol use disorder diagnosis may be useful to identify young adults with some kind of alcohol use disorder, identifying more specifically what subtype of alcohol use disorder an individual fits would enhance precision medicine and help programs better tailor treatment to meet the needs of specific sub-groups.
For scientists:Receiving an alcohol use disorder diagnosis can be a critical step in facilitating appropriate supports and treatment and limiting future harms. However, the heterogeneity in in alcohol involvement, impairment, and symptoms, among individuals with alcohol use disorder makes establishing more specific clinical guidelines difficult. This study presents a way (latent class analysis) of establishing symptom clusters. Future studies could build upon this study by recruiting a more diverse sample, particularly with more age and racial/ethnic diversity. Similarly, results may also differ across geographic and clinical settings. Cultural norms, expectancies, and supports may alter the presentation of symptoms and typologies. Methodological studies that balance diagnostic sensitivity and specificity seem needed to identify individuals with alcohol use disorder as well as demarcate clinically relevant typologies. Also unknown is how robust these types are as stable phenotypes or represent dynamic phases of the disorder at least for some.
For policy makers: Alcohol use disorder can be a crucial first step to receiving treatment and reducing harm. This study found that although DSM-5 alcohol use disorder diagnostic category requires only 2 symptoms from 11 to be met included in the category its simple summing of endorsed symptoms to arrive at clinically meaningful and medically responsive subtypes may not be the best way to identify the severity of an alcohol use disorder and which approaches to take. More funding to support methodological exploration of the dynamic clinical course of alcohol use disorder could inform clinical care and public health interventions.
Alcohol is responsible for 140,000 deaths annually in the US. Finding more effective treatments for alcohol use disorder has remained a top clinical and public health priority. For almost 100 years there have been documented clinical and public health efforts to identify different “subtypes” of “alcoholics” and other addicted persons to try to arrive at more precise treatment matches for more specific sub-groups and thus more effective treatments. Many clinicians and researchers have provided various typologies based on careful clinical observation or data-driven statistical modeling approaches. See work by Silkworth, Jelllinek, Cloninger, Babor, Hesselbrock, and Moss as stand-out examples. Such groupings have produced some interesting and compelling typologies, but these have failed to deliver on the promise of identifying robust and clinically meaningful subtypes that can lead to enhancements in “precision medicine”.
Alcohol use disorder is classified currently as a single dimensional disorder with mild, moderate, and severe subclassifications based solely on a simple sum of the number of symptoms met from a total of 11 possible symptoms. These simplified quantitatively-based subclassifications, however, may miss important qualitative differences in the impact of alcohol use disorder and how best to treat it. Similar to other attempts over the years, this study analyzed the most recent DSM-5 alcohol use disorder criteria classification to see whether certain types of symptoms naturally seem to cluster together in the hope of uncovering more meaningful diagnostic sub-groupings than merely “mild”, “moderate”, and “severe” based only a simple sum of any of 11 symptoms. The ability to identify more meaningful and similar sub-groups of individuals with the disorder may help improve treatment response by tailoring and matching treatments to these different sub-groups’ needs – often referred to as “precision medicine”.
Identifying more meaningful typologies of alcohol use disorder than ones merely based on simple sums of symptoms might be especially relevant for young adults. Young adults aged 18 to 25 tend to have the highest prevalence of past 30-day binge and heavy alcohol use as well as alcohol use disorder compared to any other age-group across the life course. In 2020, 31.4% reported binge drinking and 8.6% reported heavy alcohol use compared to 22.9% and 6.7% respectively among adults 26 and older. Given these high rates of harmful/hazardous use and alcohol use disorder, this age-range is a useful one in which to study these phenomena. Identifying, for example, who might be at greater risk for persisting alcohol use disorder versus have a subtype that may be more context-specific (e.g., due to being in a heavy drinking environment, such as college) based on an actual experiential clustering of certain symptoms, could help tailor and better match interventions to these specific sub-groups’ needs. The present study sought to investigate alcohol use disorder typologies in young adults and examine the unique protective and risk factors associated with different typologies.
HOW WAS THIS STUDY CONDUCTED?
This cross-sectional study used a convenience sample of 1,390 young adults (18-30 years old). Participants were recruited through flyers, business cards posted in the community, and posting on the Indiana University classifieds webpage. A wide variety of alcohol problems, from no problems to severe problems, were sought. Individuals were excluded if they had an externalizing disorder, which are characterized by maladaptive behaviors directed toward an individual’s environment (e.g., conduct disorder), without the presence of alcohol use disorder. Participants could, however, have alcohol use disorder in addition to another externalizing disorder. All participants completed a collection of measures to determine DSM-5 alcohol use disorder diagnosis (along with other substance use disorders), alcohol use disorder symptoms, acute alcohol use problems, treatment seeking, alcohol and other substance use, conduct disorder symptoms, anxiety, depression, borderline personality disorder, experience seeking, and impulsivity. The study used a statistical technique called latent class analysis to identify if there were naturally occurring clusters of alcohol use disorder symptoms and then investigated if these clusters were associated with individual characteristics (experience seeking, anxiety, etc.).
The final sample of 1,390 young adults included an over-representation of alcohol problems with 65% meeting DSM-5 criteria for alcohol use disorder. Additionally, 40% of the sample meet criteria for cannabis use disorder and 18% meet criteria for another substance use disorder. Participants’ age ranged from 18 to 30 years old and were 21 years old, on average. The sample was 48% female and 78% White.
WHAT DID THIS STUDY FIND?
Four symptom clusters indicated a general continuum of severity, yet were qualitatively different.
Analysis of alcohol use disorder symptoms revealed four theoretically and empirically supported clusters. These were labeled as: ‘Low Problems’, ‘Heavy Consumption’, ‘Consumption and Loss of Control’, and ‘Consumption, Loss of Control, and Withdrawal’. The classes represented 34%, 26%, 31%, and 9% of the sample respectively. The results showed an additive pattern of increasing severity. However, this pattern was not linear. Each of the classes represented a qualitatively different cluster of symptoms.
Individuals in the ‘Heavy Consumption’ group were more likely to report more frequent, higher quantities, and more binge days of alcohol use compared to those in the ‘Low Problems’ grouping. However, alcohol use did not vary between the two highest severity groups – ‘Consumption and Loss of Control’ and ‘Consumption, Loss of Control, and Withdrawal’. Those in the ‘Heavy Consumption’ group were more likely to exhibit the experience-seeking trait. There was little to no difference in the occurrence of depression between the groups, but anxiety was more likely in the two highest severity groups. Substance use other than alcohol increased in a linear fashion such that individuals in each subsequent severity group were more likely to report additional substance use. Similarly, impulsivity, conduct problems, and borderline personality traits all were more likely to be endorsed in subsequent severity groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Overall, this study of 1,390 young adults found that alcohol use disorder symptoms tended to cluster together into three groups. These findings partially support the conceptualization of alcohol use disorder as it appears in the DSM-5. The clusters did represent increasing severity: ‘Low Problems’, ‘Heavy Consumption’, ‘Consumption and Loss of Control’, and ‘Consumption, Loss of Control, and Withdrawal’. However, each cluster had a unique symptom profile as represented by the cluster name, such that each sequential group added a new cluster of symptoms (e.g., heavy consumption then loss of control then withdrawal). Individuals in the ‘Low Problems’ group reported fewer drinks, less frequent drinking, and less binge drinking as well other risks and difficulties (e.g., other drug use, impulsivity, conduct symptoms, depression) compared to the other groups. The ‘Heavy Consumption’ group reported more problems and alcohol use compared to the ‘Low Problem’ group, but fewer and less frequent drinks and problems compared to the other two groups. The amount and frequency of alcohol use, however, did not differ between the two later groups. Conversely, the ‘Consumption, Loss of Control, and Withdrawal’ group reported more difficulties and risks (e.g., acute alcohol problems, drug use, conduct symptoms, impulsivity, anxiety, and borderline personality traits) compared to all other groups. The higher likelihood of impairment in this group suggests that those individuals might require the most acute and extensive support services compared to the other groups. This study suggests that conceptualizing alcohol use disorder symptoms as having three subscales measuring consumption, loss of control, and withdrawal might possibly be more useful for developing interventions, treatment, and policy.
The existing formulation of alcohol use disorder requires endorsement of any 2 symptom criteria. However, this study shows that which symptoms an individual endorses might be useful in determining alcohol use disorder severity.
For example, alcohol consumption appears to be useful in identifying those with and without alcohol use-related problems, yet it does not distinguish between the two groups with the highest severity. This pattern is consistent with other research showing that consumption symptoms have lower predictive power compared to other symptoms. Conversely, the endorsement of symptoms related to withdrawal almost exclusively appeared in the most severe group. Identifying which group an individual most closely resides in might aid treatment planning. For example, those in the ‘Heavy Consumption’ group are less impaired, yet they are more likely to endorse the experience-seeking trait. Those in this group might benefit most from education and harm reduction strategies. On the other hand, those in the highest severity group might require physiological stabilization (e.g., medications to manage withdrawal) prior to other forms of treatment.
These findings suggest that the variation among individuals diagnosed with alcohol use disorder might be conceptualized as including three subtypes related to consumption, loss of control, and withdrawal. This conceptualization, although representative of increasing severity like alcohol use disorder’s current diagnostic system, may be more useful in treatment planning and policy making compared to the existing mild, moderate, and severe subclassifications that appear in the DSM-5 that is based merely on a sum total of the number of symptoms met. These typologies of alcohol use disorder may be especially relevant for treatment planning and policy for young adults, who have disproportionally higher rates of alcohol use disorder and alcohol-related harms compared to young and older age groups.
Unknown from this study is whether such subtypes represent robust and stable patterns of alcohol use and symptoms in these individuals or whether at least some may be phases or levels of severity, problems, and impairment, that may get worse or better or otherwise morph over time – at least for some.
These data were collected from young adults 18-30 years old (average = 21.43) who mostly identified as White (78%), the findings may not generalize to individuals who are older, younger, or with different demographic characteristics.
Although the 4-class solution was the most parsimonious and theoretically meaningful solution, the analysis found a better fit with 5- and 6-class models. Although the 5- and 6-class models comprised very few individuals, a larger and more diverse sample may support additional typologies not used in this study.
BOTTOM LINE
In this study of young adults with a high prevalence of alcohol-related problems, the researchers found that individuals could be meaningfully grouped in clusters representing qualitatively different symptom groupings with increasing severity: ‘Low Problems’, ‘Heavy Consumption’, ‘Consumption and Loss of Control’, and ‘Consumption, Loss of Control, and Withdrawal’. The simple summing of any endorsed symptoms in DSM-5 to create levels of severity (i.e., “mild” “moderate” “severe”) may not actually be that useful in identifying clinically meaningful groups or typologies of individuals with alcohol use disorder. Clinicians and treatment providers would likely benefit from knowing not only if an individual is diagnosed with an alcohol use disorder but also what is the nature and impact of that disorder. Unclear from this research is how robust and stable these subtypes are and whether these do in fact represent “types” or in some cases, “phases”, of alcohol use disorder whereby alcohol-related symptoms and impairment and negative impacts all change over time.
For individuals and families seeking recovery: If you or a loved one is experiencing symptoms related to alcohol-use, it is likely beneficial to seek medical diagnosis and support. Even if you or a loved one may not be experiencing severe impairment, early screening is likely to help link to supports.
For treatment professionals and treatment systems: Although an alcohol use disorder diagnosis may signal the need for important resources (e.g., treatment, recovery supports), like any substance use disorder diagnosis there is extensive variation among individuals in the degree of alcohol involvement, impairment, and symptoms of “alcohol use disorder.” Although the DSM-5 approach to alcohol use disorder diagnosis may be useful to identify young adults with some kind of alcohol use disorder, identifying more specifically what subtype of alcohol use disorder an individual fits would enhance precision medicine and help programs better tailor treatment to meet the needs of specific sub-groups.
For scientists:Receiving an alcohol use disorder diagnosis can be a critical step in facilitating appropriate supports and treatment and limiting future harms. However, the heterogeneity in in alcohol involvement, impairment, and symptoms, among individuals with alcohol use disorder makes establishing more specific clinical guidelines difficult. This study presents a way (latent class analysis) of establishing symptom clusters. Future studies could build upon this study by recruiting a more diverse sample, particularly with more age and racial/ethnic diversity. Similarly, results may also differ across geographic and clinical settings. Cultural norms, expectancies, and supports may alter the presentation of symptoms and typologies. Methodological studies that balance diagnostic sensitivity and specificity seem needed to identify individuals with alcohol use disorder as well as demarcate clinically relevant typologies. Also unknown is how robust these types are as stable phenotypes or represent dynamic phases of the disorder at least for some.
For policy makers: Alcohol use disorder can be a crucial first step to receiving treatment and reducing harm. This study found that although DSM-5 alcohol use disorder diagnostic category requires only 2 symptoms from 11 to be met included in the category its simple summing of endorsed symptoms to arrive at clinically meaningful and medically responsive subtypes may not be the best way to identify the severity of an alcohol use disorder and which approaches to take. More funding to support methodological exploration of the dynamic clinical course of alcohol use disorder could inform clinical care and public health interventions.