
Navigating inpatient care with opioid use disorder: Treatment pathways and their relationship to overdose
Inpatient treatment is one of the most commonly used services among opioid use disorder patients, but relatively little is known about how opioid use disorder patients navigate inpatient systems of care or how various levels of inpatient care relate to opioid overdose. This study reveals potential areas for improvement within inpatient tiers of care, finding that the majority of individuals who engage in inpatient detoxification fail to transition to longer-term inpatient treatment and ultimately return to detoxification, and that those who do seek higher levels of care may be at increased risk of overdose when transitioning between treatments.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Inpatient treatment consists of many levels of care, from acute, medically managed withdrawal – often called detoxification, or “detox” – to long-term residential treatment, and is one of the most common therapeutic settings utilized by individuals with opioid use disorder.
Despite a lack of convincing evidence for its effectiveness in treating opioid use disorder, use of inpatient treatment services among opioid use disorder treatment seekers has increased in recent years; whereas 38% of treatment seekers utilized inpatient services between 2004 and 2008, more than half of them (52%) used inpatient treatment between 2009 and 2013.
Modern day opioid research has largely focused on outpatient treatment. Relatively less is known about how opioid use disorder patients navigate the inpatient treatment system, which was in large part originally designed to cater to alcohol use disorder patients. Given the ongoing overdose crisis, it is essential to characterize all treatment pathways, including those that rely on the inpatient systems of care, and how different pathways relate to overdose prevalence and risk. Overdose is particularly important to assess in the context of inpatient detoxification services because periods of sustained abstinence result in decreased tolerance to opioid’s effects so that if someone returns to opioids using similar amounts to those used before detoxification, it can result in overdose. In an effort to better understand inpatient service use among opioid use disorder patients and its relationship to overdose, the current study characterized service use for three tiers of inpatient care, transitions between them, and overdose risk relative to the timing of a given stage of care.
HOW WAS THIS STUDY CONDUCTED?
The authors conducted a retrospective study to examine overdose and service use transitions following an inpatient detoxification episode. Analyses involved a subset of data from the Massachusetts Public Health DataWarehouse, which is overseen by the state’s Department of Public Health and includes Massachusetts residents who had health insurance (public or private) at the time of evaluation. It is worth noting that Massachusetts has a generous public option for insurance, and requires that all citizens possess health insurance, resulting in the highest proportion of insured individuals in the United States (97%). Individuals in this dataset were included in the study if they were admitted to inpatient detoxification between January of 2013 and September of 2015 and if opioids were indicated as one of their top three primary substances.
The researchers prospectively tracked admissions/transitions to subsequent levels of inpatient care, as well as fatal/non-fatal overdoses, until re-admission to inpatient detoxification or the end of the database in 2015. The research team ultimately assessed three tiers of care, including:
- Inpatient detoxification (typical duration: 3-7 days): Medically monitored/managed intensive inpatient services staffed by addiction treatment, mental health, and general medical professionals who provide 24-hour treatment, nursing care, medication to manage acute withdrawal, physician and counselor availability for supporting detoxification;
- Post-detoxification treatment services (typical duration: 10-30 days): Clinically managed high-intensity residential services staffed by addiction treatment, mental health, and general medical professionals that offer 24-hour care and transitional support services (e.g., case management) aimed at stabilizing and preparing patients for transitions to other stages of care;
- Residential treatment (typical duration: 6 months – 2 years): Clinically managed low-intensity residential services that provide 24 hour living support, structured individual/group counseling, recovery support activities, and support for re-entry to the general community (e.g., employment services).
Outcomes of interest included treatment exit at each stage of care, transitions to other levels of inpatient treatment, overall overdose prevalence and risk, as well as the timing of overdose relative to an exit from care, and the risk of overdose relative to the last stage of care received.
Treatment exit was defined as any discharge from inpatient treatment in the dataset (could reflect a medically-appropriate exit from completed care, but also includes the possibility of returning to substance use, not seeking additional care, seeking outpatient care, seeking inpatient care outside the Massachusetts public health department’s system, moving outside of Massachusetts, etc.). Progressions from inpatient detoxification to other levels of care, as well as re-admissions to detoxification, were defined as admissions occurring after a given detoxification episode. The researchers calculated the number of fatal and non-fatal overdoses that occurred during periods of transition between levels of care and after exiting a given level of care without further treatment, as well as the opioid overdose rate per 100 person years (number of overdoses, taking into account the number of people in the study and the amount of time each person contributes to the study, which standardizes measures across different people). The influence of demographics on overdose risk was also evaluated. The final dataset included 81,519 admissions to inpatient detoxification.
WHAT DID THIS STUDY FIND?

Figure 1. The figure above depicts the various treatment pathways of individuals who utilized inpatient detoxification services. Percentages reflect the proportion of individuals who followed a given treatment path, out of the entire sample (N=81,519).
The majority of detoxification episodes only involve detoxification – with no further treatment – and a minority of those who engaged attended long-term residential treatment.
More than three-fourths of detoxification episodes (76%) consisted only of detoxification – that is, individuals were discharged without entering a higher level of care. After leaving detoxification, 51% were subsequently re-admitted to detoxification and 25% did not receive any additional care.
The remaining 24% of individuals who were discharged from detoxification received further care. Twenty percent transitioned to post-detoxification treatment and 4% transitioned directly to residential treatment.
Of the 15,816 individuals who used post-detoxification treatment services, 47% were discharged without subsequent treatment, 36% were discharged and then re-admitted to inpatient detoxification, and 17% subsequently transitioned to residential treatment (i.e., 9%, 7%, & 4% of total sample, respectively).
Of the 6,163 individuals admitted to residential treatment (8% of total sample), 70% were discharged without subsequent treatment and 30% were re-admitted to inpatient detoxification (i.e., 5% and 3% of total sample, respectively).
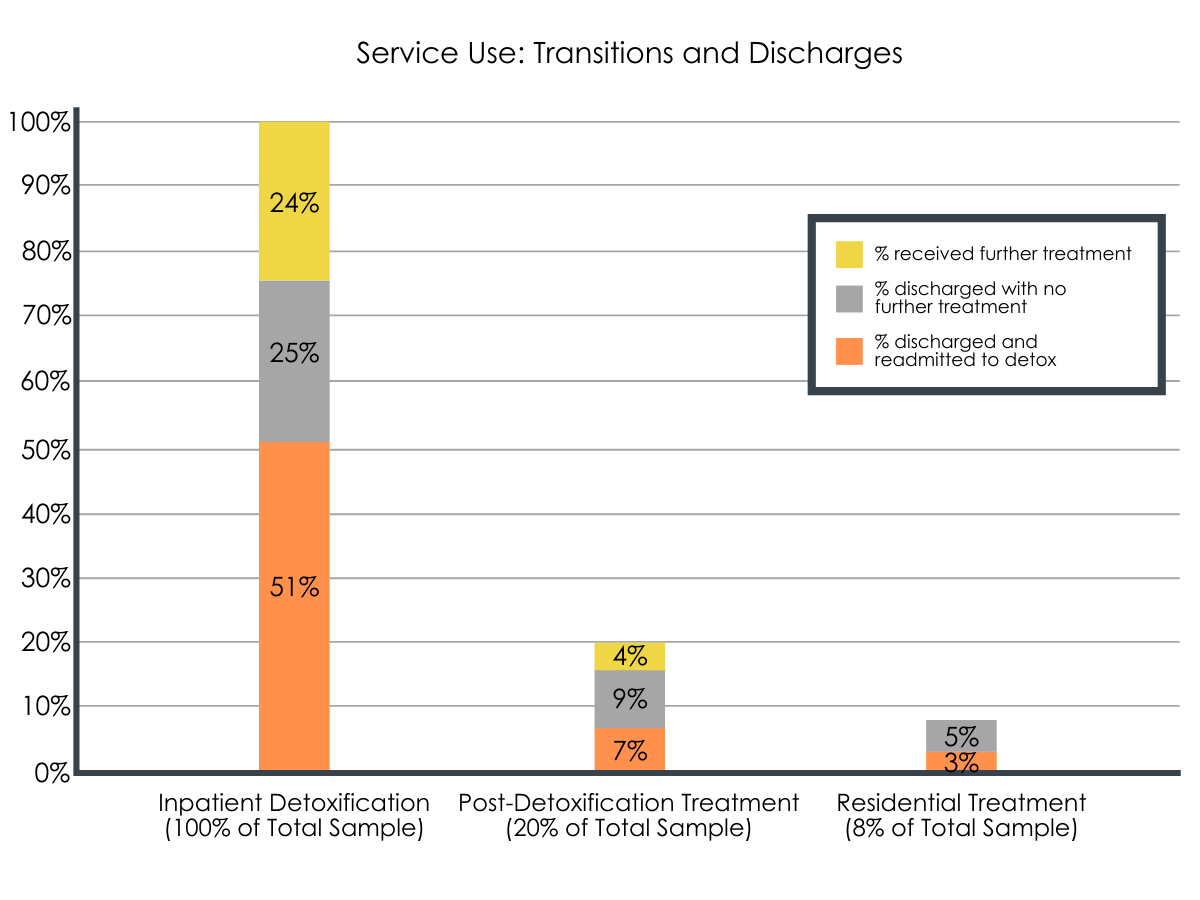
Figure 2. Depicts the prevalence of service use, discharge, transition to other treatment services, and return to detoxification at 3 levels of care (i.e., inpatient detoxification, less intensive post-detoxification treatment, and low-intensity residential treatment). Bars depict the total percentage of individuals who utilized each of the 3 levels of care. Percentages within bars reflect post-discharge pathways (i.e., re-admitted to inpatient detoxification, discharged without further treatment, transitioned to a higher level of care) among the entire sample, after undergoing a given treatment.
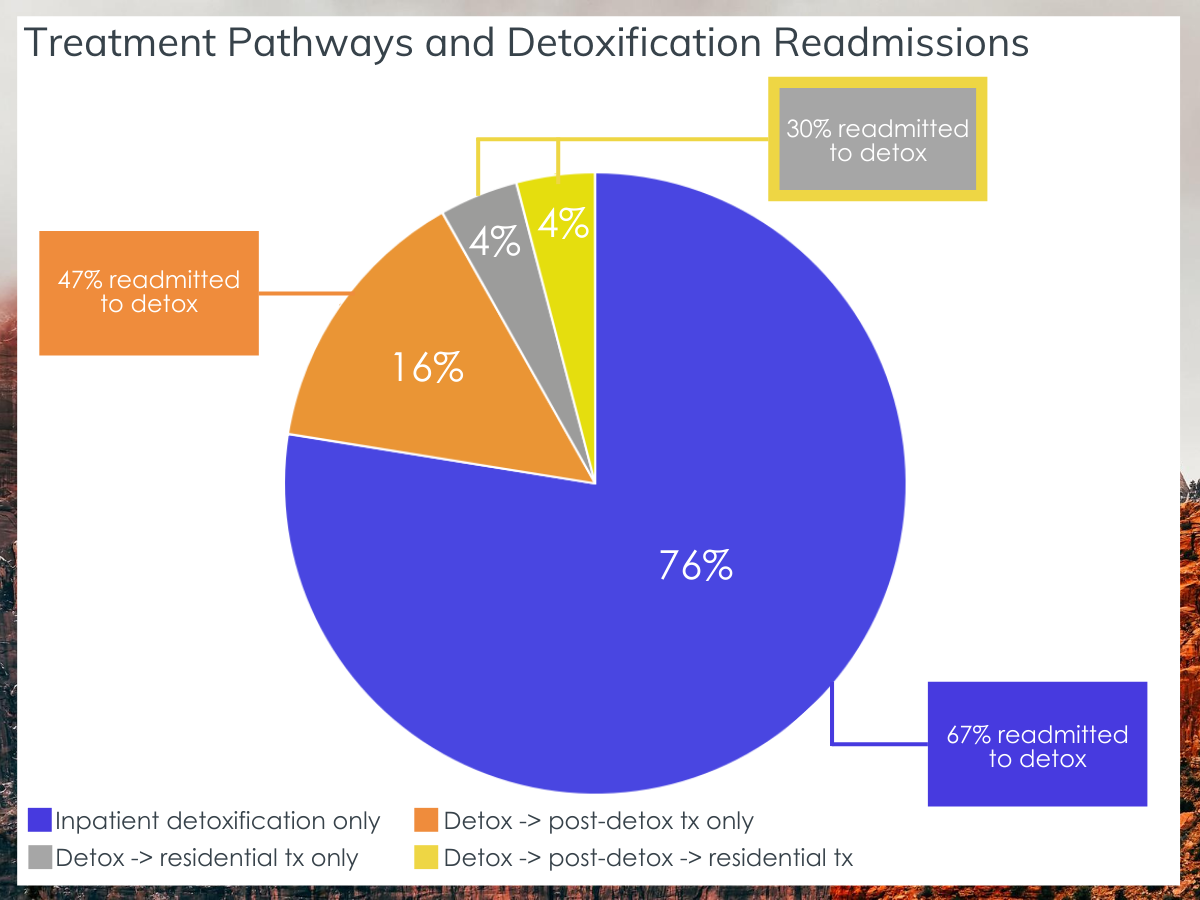
Figure 3. Pie chart depicts the treatment pathways that individuals took, including the percentage of those who attended detoxification only, and those who transitioned to various stages of subsequent care. Call-out boxes display the percentage of those in specific treatment categories that were re-admitted to detoxification post discharge from that level of care (e.g., 67% of those who received inpatient detoxification without further care were ultimately re-admitted to inpatient detoxification).
Risk of any overdose was highest when patients were transitioning between stages of care and rates of fatal overdose were most common when post-detoxification care was not received.
Nine percent of all inpatient detoxification episodes were followed by an opioid-related overdose at some point during the study period (i.e., 7,624 overdoses). In general, this number translates to 13.4 overdose events per 100 person years. Of the 7,624 overdose episodes, 4% resulted in a fatality. Fatal overdose most commonly occurred following discharge from inpatient detoxification without any further care (77%).
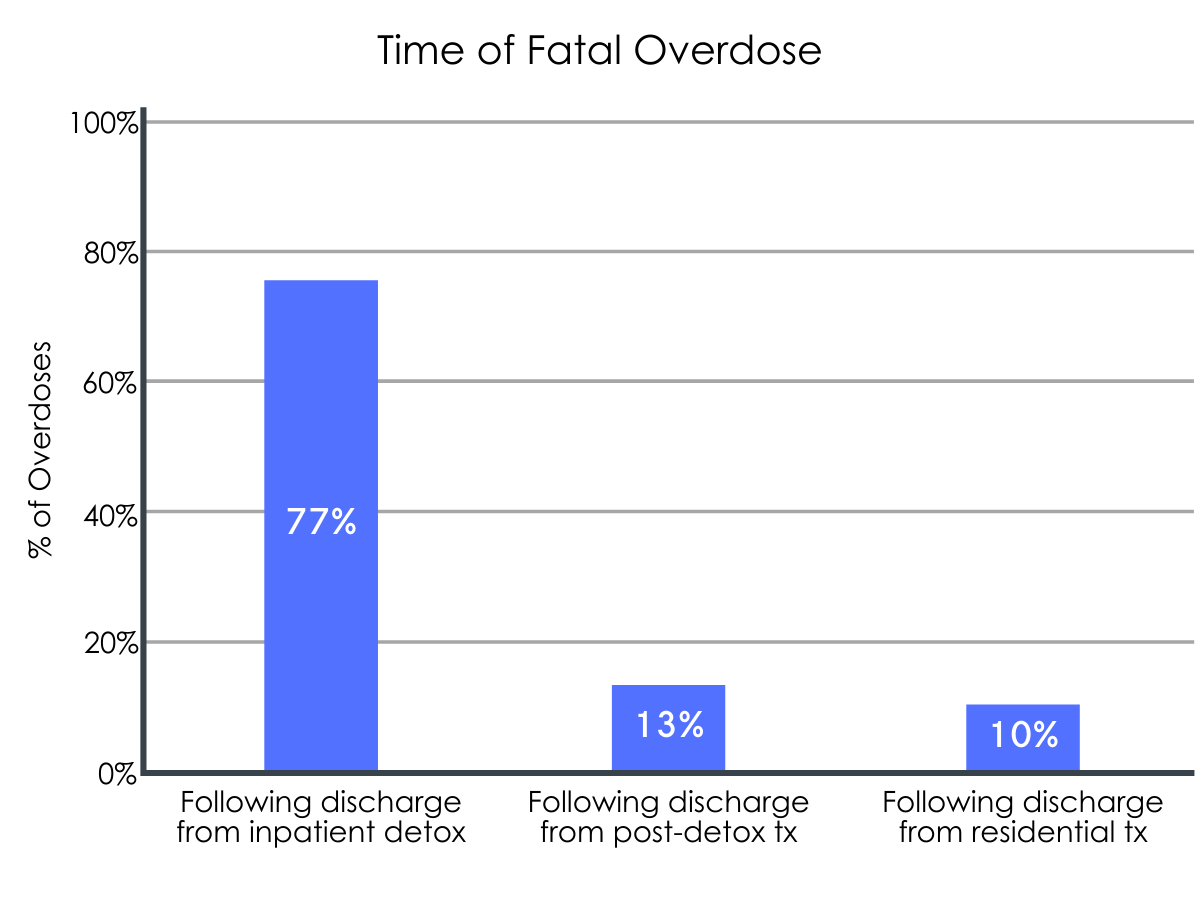
Figure 4. Depicts the percentage of all fatal overdoses that occurred after discharge from a given stage of care.
General risk of overdose (fatal or non-fatal) was highest during periods of transition from inpatient detoxification to post-detoxification treatment (55.1 overdoses per 100 person years) and lowest following discharge from residential treatment (6.6 overdoses per 100 person years) and post-detoxification treatment (5.9 overdoses per 100 person years).

Figure 5. Illustrates overdose risk at different stages of care and transitions between them. The overall overdose rate (depicted in grey) offers a reference point for risk.
Overdose rates were proportionally much higher just after discharge from treatment and overdose risk varied by patient characteristics.
Ninety-two percent of all overdoses occurred after a treatment discharge. For all levels of care (i.e., detox, post-detox, residential), the highest rates of overdose were observed just after exiting treatment, with about 20% of overdoses occurring within just 14 days of discharge. When considering longer time intervals, about 40% of overdoses occurred between four months and 1.5 years after discharge. Risk of overdose varied by gender, race, ethnicity, and mental health status. Men, non-Hispanic White individuals, and individuals undergoing treatment for a comorbid mental health condition exhibited increased risk of overdose (15, 16, and 15 overdoses per 100 person years, respectively). Conversely, decreased risk of overdose was observed for women, non-Hispanic black and Hispanic individuals (11, 5, and 8 overdoses per 100 person years, respectively).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand opioid use disorder treatment pathways and highlight areas for improving therapeutic approaches in the inpatient sector. By evaluating how patients navigate the treatment system, this study speaks to potential avenues for enhancing a somewhat outdated and largely alcohol-focused tier of care to ultimately help address the opioid overdose epidemic. The research team found that progression through all stages of inpatient treatment (inpatient detoxification à post-detoxification treatment à residential treatment) was uncommon, with the majority of individuals leaving care after inpatient detoxification.
Consistent with national statistics of treatment utilization, only 25% of detoxification episodes were followed by transitions to other inpatient treatment services.

Figure 6.
The majority of these individuals transitioned from inpatient detoxification to post-detoxification treatment. A much smaller percentage of individuals transitioned to residential treatment (8%). It is unclear why so few patients utilized long term residential treatment – though barriers to treatment entry could play a role, long term residential treatment also imposes significant lifestyle changes that are likely to disrupt many facets of daily living (e.g., work, family, housing). This level of commitment may be unappealing to some individuals and others may be better suited for less intensive treatment (e.g., outpatient) after inpatient detoxification.
Still, inpatient detoxification episodes in the current study didn’t necessarily have to be completed – transitions to other forms of inpatient care often require completion of detoxification and any individuals who were unable to complete a detoxification episode (e.g., prematurely discharged) may not have had the opportunity to transition to higher levels of care. Studies suggest that about half of opioid use disorder patients drop out of inpatient detoxification and high rates of return to substance use are reported among individuals who fail to receive continuing care after detoxification. Consistently, this study revealed that the majority of individuals who received inpatient detoxification, without further care, eventually return to detoxification. Indicative of relapse to active, opioid use disorder, these findings underscore the point that inpatient detoxification services are very rarely adequate as a standalone treatment for opioid use disorder.
Detoxification discharge also constitutes a period of heightened risk for overdose, such that returning to opioid use in amounts similar to those used before detoxification can result in overdose due to decreased physiological tolerance. Accordingly, this study found that a disproportionate number of overdoses occurred in close (≤14 days) proximity to discharge from all levels of care and fatal overdose most commonly occurred after discharge from inpatient detoxification, suggesting periods of heightened vulnerability just after a treatment discharge and highlighting the importance of continued care and recovery support after completing a treatment episode, particularly detoxification.
When the authors looked at general overdose risk, they found the highest risk during periods of transition from inpatient detoxification to post-detoxification treatment. Interestingly, discharge from inpatient detoxification (without further treatment) was only associated with a moderately increased overdose risk. Severity of disorder may play a role in these findings, such that those individuals who sought further care may have had more severe opioid use disorders.
Although discharge at the post-detoxification and/or residential treatment level predicted the lowest risk of overdose, transition periods between levels of care (i.e., from inpatient detox à post-detox treatment à residential treatment) were identified as periods of significant overdose risk. Individuals transitioning to higher levels of care might experience long wait times, and a delayed transition to follow-up care could pose significant risk for a return to substance use and subsequent overdose pending admission.
In the current study, average wait times were about 15 days between transitions. This finding demonstrates the importance of timely and seamless linkage to treatment at various levels of care. Additional research is needed to identify optimal ways for enhancing operating procedures within various treatment contexts (inpatient, outpatient, community), to ultimately facilitate successful transitions through the treatment system. Developing strategies to aid transitions (e.g., motivational interviewing, case management, connections to mutual help organizations) and providing intermittent treatment and support when transitions are delayed are essential for supporting this population and lowering overdose rates. Given that heightened overdose risk was also seen among men, non-Hispanic white individuals, and individuals with co-occurring mental health disorders, additional post-treatment support may be warranted to help protect patients with these sociodemographic and medical characteristics.
Importantly, this study did not assess transitions from inpatient care to other types of care, such as outpatient medication treatment. Medication treatment has repeatedly been shown to be the most effective therapy to reduce opioid use and overdose risk for individuals with opioid use disorder, particularly agonists like buprenorphine and methadone, which, if maintained over time (> 6 months), are superior to other treatment options like intensive behavioral or intensive outpatient treatments.

Figure 7.
Similar investigations of medical health records have demonstrated reduced risk of overall death and opioid-related overdose deaths, more specifically, among those who receive medication treatment following detoxification. Medication treatment is also associated with improved retention in treatment. Given that the majority of individuals left care after inpatient detoxification and failed to receive a higher level of inpatient care, detoxification facilities may be an ideal place to introduce medication treatment (e.g., extended-release injectable naltrexone or buprenorphine) to opioid use disorder patients, as detox may be their only point of contact with the treatment system. Initiating medication treatment in the context of a detoxification facility and subsequently linking patients to longer-term medication treatment providers in a timely manner could ultimately help mitigate the opioid overdose epidemic and facilitate patients’ successful recovery. Although the current study did not track transitions to outpatient psychosocial or medication treatment, the high rate of return to inpatient detoxification suggests there may be a significant number of people who are not utilizing outpatient and community-based services, and they could potentially benefit from being offered alternative therapeutic approaches, like medication treatment, in the context of a detoxification facility.
- LIMITATIONS
-
- This research was based on a dataset of Massachusetts residents and may not generalize to other geographic regions, as overdose and treatment availability may also be affected by healthcare systems, harm reduction programs, and treatment/recovery support services offered in a given region. This study did not assess transitions from inpatient to outpatient care, which accounts for a large percentage of opioid use disorder patients. The authors did not account for addiction severity, treatment duration, or those who received medication treatment services (e.g., buprenorphine, methadone, injectable naltrexone), which is shown to influence treatment retention/outcomes, warranting further investigation. Patients also self-selected their post-detoxification plans, which could lead to individual differences not accounted for in this study.
- The analyses were based on a cumulative state healthcare dataset, heightening risk for misreported or undocumented treatment episodes. In addition to those in recovery, treatment discharge without further care may have included individuals who had returned to substance use, moved out of MA state, sought additional treatment in a residential facility not included in the current study’s database, or who were referred to an outpatient treatment provider, which could ultimately influence study outcomes regarding treatment discharge and overdose timing.
- Individuals included in this study had opioids designated as one of their top three drugs of choice. Therefore, opioids may not be the primary substance used by all participants. Timing of fatal overdose was assessed based on the last treatment episode in the database, which may not accurately reflect the last episode of care received. Moreover, discontinuation was defined as the end of a treatment episode without mention of whether or not that treatment was completed. Additional research is needed to determine the influence of other treatment modalities and recovery services on overdose and return to care, and to examine the influence of treatment duration/completion.
BOTTOM LINE
- For individuals and families seeking recovery: Studies like this help us better understand how opioid use disorder patients navigate the treatment system and how different treatment pathways relate to overdose. Focusing on the inpatient treatment, this study found that most opioid use disorder patients who enter inpatient detoxification leave without receiving a higher level of care (i.e., post-detoxification inpatient treatment or residential treatment) and ultimately return to substance use and detoxification, and that navigating care in this way is associated with increased risk of overdose. Overdose risk was also high when individuals were transitioning between different treatment types (e.g., from inpatient detox -> post-detox treatment). These findings emphasize the importance of ongoing care after detoxification and seamless transitions between various stages of treatment. With only one-quarter of individuals receiving follow-up care, inpatient detoxification is the only type of treatment that many patients encounter. Individuals considering inpatient detoxification for opioid use disorder should talk to their treatment providers about how the detoxification episode fits into their overall ongoing treatment and recovery plan to aid successful transition and enhance the chances of remission and reduce overdose risk. Medication treatment (e.g., methadone, buprenorphine) has shown to be the most effective therapy for opioid use disorder and can reduce risk of overdose after detoxification. Therefore, pairing inpatient detoxification with medication treatment services and linkage to community-based providers could ultimately help enhance recovery outcomes and reduce risk of overdose.
- For treatment professionals and treatment systems: Studies like this help us better understand how opioid use disorder patients navigate the treatment system and its relationship to overdose. Focusing on the inpatient sector of care, the authors found that most individuals enter inpatient detoxification without entering higher levels of care (post-detoxification & residential treatment), and that the majority of these individuals eventually return to inpatient detoxification, suggesting high rates of relapse or return to substance use. Fatal overdose was most common after discharge from detoxification, emphasizing the importance of receiving ongoing care after a decrease in physiological tolerance for opioids. Furthermore, it took an average of ~15 days for patients to transition to post-detoxification or residential treatment, and general overdose risk was highest during these transition periods, highlighting the need for timely and seamless linkage to treatment at various levels of care. With only 24% of patients receiving follow-up care, it may be worthwhile to expand the services offered by inpatient detoxification. Medication treatment (e.g., methadone, buprenorphine) is one of the most effective therapies for opioid use disorder and can reduce risk of opioid overdose after detoxification. Therefore, detoxification facilities may be an ideal place to introduce medication treatment to patients, as detox may be their only point of contact with the treatment system. Offering additional services in detoxification and subsequently linking patients to longer-term medication treatment providers in a timely manner could ultimately help mitigate the opioid overdose epidemic and enhance treatment outcomes.
- For scientists: This retrospective study examined the inpatient treatment pathways of opioid use disorder patients and the relationship between different treatment pathways and overdose. The authors found that the majority of individuals who enter inpatient detoxification do not receive higher levels of care (post-detoxification inpatient treatment & residential treatment) and most individuals eventually return to inpatient detoxification, indicating high rates of relapse or a return to substance use. Fatal overdose was highest following an inpatient detoxification discharge and overdose risk was highest during periods of transition from inpatient detoxification to post-detoxification treatment and from post-detoxification to residential treatment, emphasizing the importance of receiving ongoing care in the context of depleted opioid tolerance, and of timely and seamless linkage to treatment at various levels of care. Given that inpatient detoxification is the only point of contact with the treatment system for many opioid use disorder patients, it may be necessary to reevaluate the services offered to them at the detoxification level of care. Additional research is needed to investigate outcomes at the national level, transitions between inpatient and outpatient care, the effects of expanding inpatient detoxification services (e.g., incorporating medication treatment with buprenorphine), and novel methods for facilitating transitions between levels of addiction treatment to mitigate opioid overdose and facilitate treatment/recovery outcomes.
- For policy makers: Studies like this help us better understand how opioid use disorder patients navigate the treatment system and how it relates to overdose risk. Focusing on the inpatient sector of care, this study reveals that most opioid use disorder patients who enter inpatient detoxification exit the treatment system without further care, and that navigating care in this way is associated with heightened risk of overdose. This is because opioid tolerance diminishes during detoxification, increasing one’s risk of overdose should they return to substance use. Given high rates of recurrence of substance use and return to detoxification, with only about one-quarter of patients receiving higher levels of care (residential treatment or post-detoxification inpatient treatment), detoxification facilities may be an ideal setting to introduce and link patients to continued care. Overdose risk was also heightened during periods of transition between levels of care, revealing a potential need to enhance coordination and transition between different treatment sectors. Additional funding for research will help characterize transitions from inpatient detoxification to other treatment/recovery sectors (e.g., outpatient), and to identify beneficial therapies within detoxification facilities (e.g., medication treatment) and novel methods for facilitating treatment transitions and outcomes, which can ultimately reduce rates of relapse, repeated use of detoxification services, and overdose. Further research in states with different healthcare systems, including those with less universal insurance and access to care, will be essential for determining if these findings generalize outside of Massachusetts.
CITATIONS
Morgan, J. R., Wang, J., Barocas, J. A., Jaeger, J. L., Durham, N. N., Babakhanlou-Chase, H., … & Linas, B. P. (2020). Opioid overdose and inpatient care for substance use disorder care in Massachusetts. Journal of Substance Abuse Treatment, 112, 42-48. doi: 10.1016/j.jsat.2020.01.017