
Outpatient Treatment & Recovery Residences: How Do Clients Do Over Time When The Services Are Offered Together?
Outpatient treatment is the most frequently used level of care for substance use disorder. This means, that patients return home at night, often to treacherous living environments that may increase relapse risk. This study examined the long-term outcomes for clients who combined outpatient treatment services with recovery residences.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Outpatient care for substance use disorder is now the most common level of treatment intensity in the U.S.. Inpatient or residential settings have diminished over the past several decades which have helped with healthcare cost containment but have left the most vulnerable clients exposed to environmental risks that encourage potentially lethal substance use. Relapse rates are high for clients who do not live in environments that support recovery and the progress they make while attending outpatient treatment can be lost or compromised. There is a need for more research on alcohol and drug free housing for clients who are involved in outpatient treatment. This study fills this gap by testing the degree to which recovery residences, combined with outpatient treatment, represent a pathway to recovery along the continuum of care for substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
The authors examined changes over time for each of the following outcome measures:
- legal problems
- employment
- peak density of substance use (i.e., number of substance use days during the month of highest use over the past 6 months)
- abstinence (yes or no)
- arrests
- alcohol and other drug use
- family problems
- medical problems
- psychiatric problems
Specifically, they tested to see if the outcome measures improved between baseline and 6 months, and if areas of improvement were maintained at 12 and 18 months.
The authors hypothesized that all outcomes measures with high severity scores at baseline would show significant improvements at 18 months, and low severity scores would maintain low severity at 18 months. In addition, recovery-related correlates (12-step involvement and alcohol or other drug use in social network) were examined with outcome measures.
Study participants consisted of 55 individuals entering four different recovery residences that were operated by Options Recovery Services in California. The participants were interviewed during their first week as residents between 2004-2006 and interviewed again at 6 months (86% follow-up rate), 12 months (76% follow-up rate), and 18 months (71% follow-up rate). Many baseline demographic factors were controlled for in the analysis including age, race, education, marital status, gender as well as time of interview in order to estimate the effect of sober living home participation independent of these factors.
WHAT DID THIS STUDY FIND?
Average Scores for Legal Problems, Employment, Peak Density, Abstinence and Arrests Improved Over Time Compared to Baseline
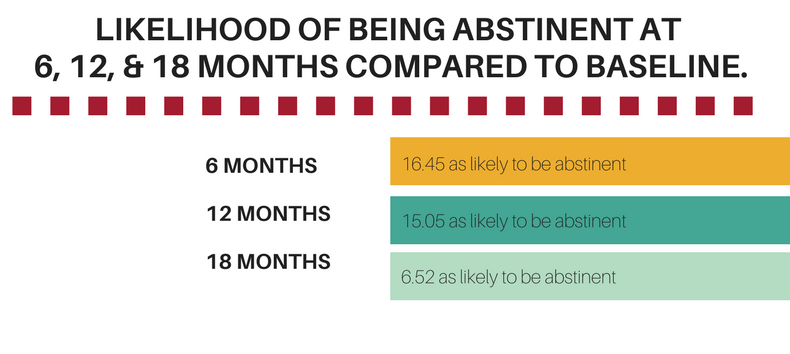
For residents, many outcome measures showed significant improvement between baseline and 6 months (i.e. legal problems, employment, peak density, abstinence, and arrests) with the exception of number of days worked. Most of these improvements persisted at 12 and 18 months relative to baseline with the exception of legal problems at 18 months. For example, at baseline 19.3 days of substance use per month was the average peak density over the past 6 months prior to entering the house. By 6 and 12 months residents were 15.4 times more likely to have fewer days of substance use during peak density and by 18 months were 10.7 times more likely compared to baseline.
See the figure below for the likelihood of being abstinent at 6, 12, and 18 months compared to baseline.
Low Scores for Alcohol and Other Drug Use at Baseline Were Mostly Maintained Over Time
As hypothesized, residents entered the recovery residences with generally low alcohol and drug use scores that were maintained at follow up time points when compared to baseline. The mean alcohol severity score was .07 (on a scale of 0-1 with 1 being worse) at baseline, .06 at 6 months, .5 at 12 months, and .11 at 18 months. The mean drug use severity core was .05 at baseline, .03 at 6 months, .05 at 12 months, and .11 at 18 months.
Higher Scores for Family Problems, Medical Problems, and Psychiatric Problems at Baseline Did Not Decrease Over Time
Counter to the hypothesis, the residence had generally high average scores on some of the non-substance use based quality of life indicators (i.e., substance use related problems) that did not decrease at follow-ups.
Recovery-related Correlates of Outcomes
Higher levels of 12-step involvement (e.g., sponsorship, spirituality, volunteer service position) were predictive of reduced days of substance use during peak density and a 25% increase in the likelihood of being abstinent over the entire 18-month study period. Furthermore, alcohol and drug use in the social network predicted increased days of substance use during peak density. Drug use in the social network predicted decrease in days worked and increased alcohol severity.
WHY IS THIS STUDY IMPORTANT?
There is a need for alcohol and drug free housing for clients who are involved in outpatient treatment for substance use disorder.
This study found that among residents entering recovery residences while completing outpatient treatment, many important indicators of recovery from substance use disorder (i.e., peak density number of substance use days and abstinence) and associated problems (legal, employment, and arrests) improved at 12 and 18 months relative to baseline. This suggests that using a sober living environment while in outpatient treatment for substance use disorder may be a pathway to recovery that can support remission and improve quality of life.
A critical question here was if progress made during treatment (e.g., 30 days of sobriety required before entering house) could be maintained and enhanced with recovery residences. The results showed no significant increase in alcohol or drug problems up to 18 months. Alternatively, residents were high on several important markers of impaired day to day functioning upon entering recovery residences, such as family, medical, and psychiatric problems, but showed no improvement on these indicators over time.
Recovery residences may offer minimal impact on these areas or alternatively, limited opportunities for improvement may exist. For example, some residents entered the home with chronic health conditions that are not easily improved such as HIV and hepatitis. Additionally, estranged family relationships may continue to have no or minimal contact even after entering the house. Targeted medical and social services are likely needed to make a substantial difference on these recovery-related outcomes.
- LIMITATIONS
-
- There was no comparison group included in the analysis so it cannot be assumed that the observed outcomes are due to recovery residences. In this study, individuals self selected into the recovery residences and the characteristics of these individuals (e.g., motivation for recovery) may have in part accounted for the longitudinal improvements. This type of design stands in contrast to a randomized controlled trial of Oxford House Residents, where the residents’ better outcomes compared to those receiving typical continuing care can be attributed to the ingredients present in those types of recovery residences, rather than some other contributor to better outcomes (e.g., high initial commitment to abstinence).
NEXT STEPS
The next steps are to test this model using a sample of women (this sample was 94% male) and using a comparison group to determine if and how women can equally benefit from recovery residences coupled with outpatient treatment.
BOTTOM LINE
- For individuals & families seeking recovery: This long-term follow up of clients who used both recovery residences and outpatient treatment for substance use disorder found that drug and alcohol use decreased over the course of 18 months compared to baseline. Furthermore, legal problems, employment, and arrests improved over time. This study had no comparison group so there is a higher degree of uncertainty if the findings were due to the recovery residence and treatment alone, but combined with other evidence, the research suggests they are likely to help. The gains in sobriety and quality of life that are achieved during treatment may be enhanced by a peer-based alcohol and drug free environment to support recovery. If you or a family member need safe housing to support your treatment goals, consider a certified recovery residence.
- For scientists: This long-term follow-up of clients in outpatient treatment who resided in recovery residences, found that client substance use can reduce over time when these two services are combined. Improvements in family, medical, and psychiatric problems, however, did not improve by 18 months. It would be useful to learn more about the tools that could be incorporated into this model to target the co-occurring problems that can hinder recovery progress from substance use disorder.
- For policy makers: There is a growing body of research suggesting that recovery residencies have the potential to be a peer-based option on the continuum of care for substance use disorder. This rare long-term study found that combining recovery housing with outpatient treatment may be an empirically supported pathway to recovery to reduce substance use and improve quality of life. Policies and funding avenues that support this line of research and increase access to recovery residences for people in treatment for substance use disorder may help address the prodigious public health burden of substance use disorder within your respective constituencies.
- For treatment professionals and treatment systems: A common challenge facing clients who receive outpatient services is finding a living environment that is free of alcohol and drugs and promotes recovery. It might be helpful to take stock of your clients’ environmental needs as part of a comprehensive treatment plan. If a stable and supportive housing arrangement is needed, arrangements with a certified recovery residence can fill that necessity and enhance treatment goals for remission and improved quality of life.
CITATIONS
Polcin, D.L., Korcha, R., Bond, J., Galloway, G. (2010). Eighteen month outcomes for clients receiving combined outpatient treatment and sober living houses. J Subst Use, 15(5), 352-366. doi:10.3109/14659890903531279