
It works, but why does it work? Perspectives on change in 12-step and non-12-step mutual-help groups
There has been substantial growth of recovery mutual-help groups that adopt non-12-step philosophies. Findings from this study suggest that these newer groups may support change in many of the same ways as 12-step groups. Better understanding how these groups work can provide more options for people with substance use disorders and inform both clinicians and policy makers in supporting people seeking recovery.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Research shows that Alcoholic Anonymous (AA) is as effective, or on some important outcomes more effective, than other psychosocial interventions in treating Alcohol Use Disorder (AUD) and also more cost-effective. For the first year of recovery, studies show that having a sponsor and participating in service each predict reduced numbers of days drinking. Greater meeting attendance also appears to increase the number of days abstinent. Other studies suggest that, while different groups (men versus women; younger versus older adults) benefit from 12–step programs in different ways, social support and transforming personal networks are ways that group participation benefits many people. A better understanding of ways that 12-step programs support individuals in maintaining a process of directed, positive, change could help recovery professionals and empower people in recovery to utilize these groups in the most impactful fashion.
The past few decades have also seen substantial growth of new mutual-help organizations such as the Self-Management and Recovery Training program (SMART), LifeRing, Women for Sobriety, All Recovery meetings, Recovery Dharma/Refuge Recovery, and a huge number of local, less formal groups. Like AA, these groups are peer-led and non-professional. They provide some of the same kinds of social support as AA and incorporate similar elements such as sharing stories in meetings. But they do not utilize the 12 steps and many of them are explicitly secular rather than spiritual. Some are religious (e.g., Celebrate Recovery). Preliminary research suggests that SMART and Women for Sobriety may be as effective as AA for those who choose to attend them, even after accounting for higher rates of initial abstinence goals among those who chose to attend AA. Researchers have not clearly established if some, or even all, of these newer mutual-help organizations are as effective as AA. Nor have researchers explored whether the same “active ingredients” or mechanisms of change that explain why AA works for many individuals are also found in other groups. It is an open question whether these groups help for the same reasons as AA, for different reasons altogether, or some combination of these two possibilities.
In this study, Rettie and colleagues surveyed 151 people who are active in 12-step and non-12-step groups in the United Kingdom. They asked if possible “active ingredients” that sustain recovery are 1) present in their group and 2) important to them. They also asked participants to write a description of their group and analyzed these responses to identify potential mechanisms of change that might not be in the existing research.
HOW WAS THIS STUDY CONDUCTED?
This was a mixed methods study evaluating the presence and perceived importance of potential mutual-help active ingredients in 151 individuals from 30 different addiction support groups across the UK grouped into one of three categories: 12-step groups; structured non-12-step groups; and unstructured non-12-step groups. In mixed methods designs, researchers combine quantitative data (which is analyzed using statistics) and qualitative data (observations or interviews analyzed to understand how individuals understand a phenomenon). This approach allows researchers to explore patterns on the scale of populations and the meaning that these patterns have for specific individuals and communities.
For this study, the research team first asked participants to answer one of two questions about their mutual-help group. They then administered a survey that requested participants 1) rank whether each of 12 behavioral “active ingredients” are present in their recovery group and 2) rank how important these aspects of group participation are to them. The narrative answers were analyzed using thematic analysis, a method that generates codes and themes from qualitative data based on induction. The research team used statistical analyses to order potential mechanisms by importance and frequency. They also tested whether there were ranking differences between these ingredients, overall, and whether different groups had different rankings (for example, if members of different groups ranked “active ingredients” differently.) In these analyses, they controlled statistically for group membership and length of time in recovery. The results were then combined to create a new list of potential mechanisms of change that participants identified as being both present and important in 12-step and non-12-step mutual-help.
The research team utilized an existing framework that suggested possible “active ingredients” of AA and other psychosocial interventions based on widely-accepted theories of how people resolved substance use problems. This framework identified 4 relevant theories from the psychological literature: social control theory; social learning theory; behavioral economics/behavioral choice theory; and stress and coping theory. Social control theory suggests the importance of bonding between group members, goals set by the group, and structure. Social learning theory suggests the importance of learning group norms and emulating role models. Behavioral economics suggest the importance of rewarding activities other than substance use. Stress and coping theory suggest the importance of building coping skills and self-efficacy to manage the stressors that lead to use.

Figure 1.
Sixty-nine percent were male, and the average age was 42.5 years. Participants were recruited through social media, flyers placed at national recovery related events, and attendance of local groups. The majority of participants were white (97%). 34% of participants stated that they had used alcohol problematically. 20% indicted that they had used drugs. 34% indicated that they had used both alcohol and drugs. Based on individual self-reports, the participants had an average time in recovery of 32.2 months (2.68 years) with a range of 1 to 462 months (38.5 years) and a standard deviation of 61.24 months (5.1 years).
WHAT DID THIS STUDY FIND?
“Active Ingredients” were identified as equally common among 12-step and non-12-step groups.
The research team found that all of the proposed mechanisms were identified as both present and important. Participants identified the 12 mechanisms as typically offered in their groups at high levels. The group’s ability to improve self-confidence was ranked as the most widely offered component (average score = 87.59 out of 100). However, the researchers concluded that “improving self-confidence” was ranked as equally common as the 5 other most highly rated components of participation: bonding; sober lifestyle; coping skills; giving back; and role models. Compared to these potential active ingredients of group participation, receiving rewards was experienced less often, although it still received a score of 78.08 out of 100, suggesting participants generally perceived it to be an active ingredient in most groups. Critically participants experienced the various active ingredients just as commonly across 12-step, structured non-12-step, and unstructured non-12-step groups.
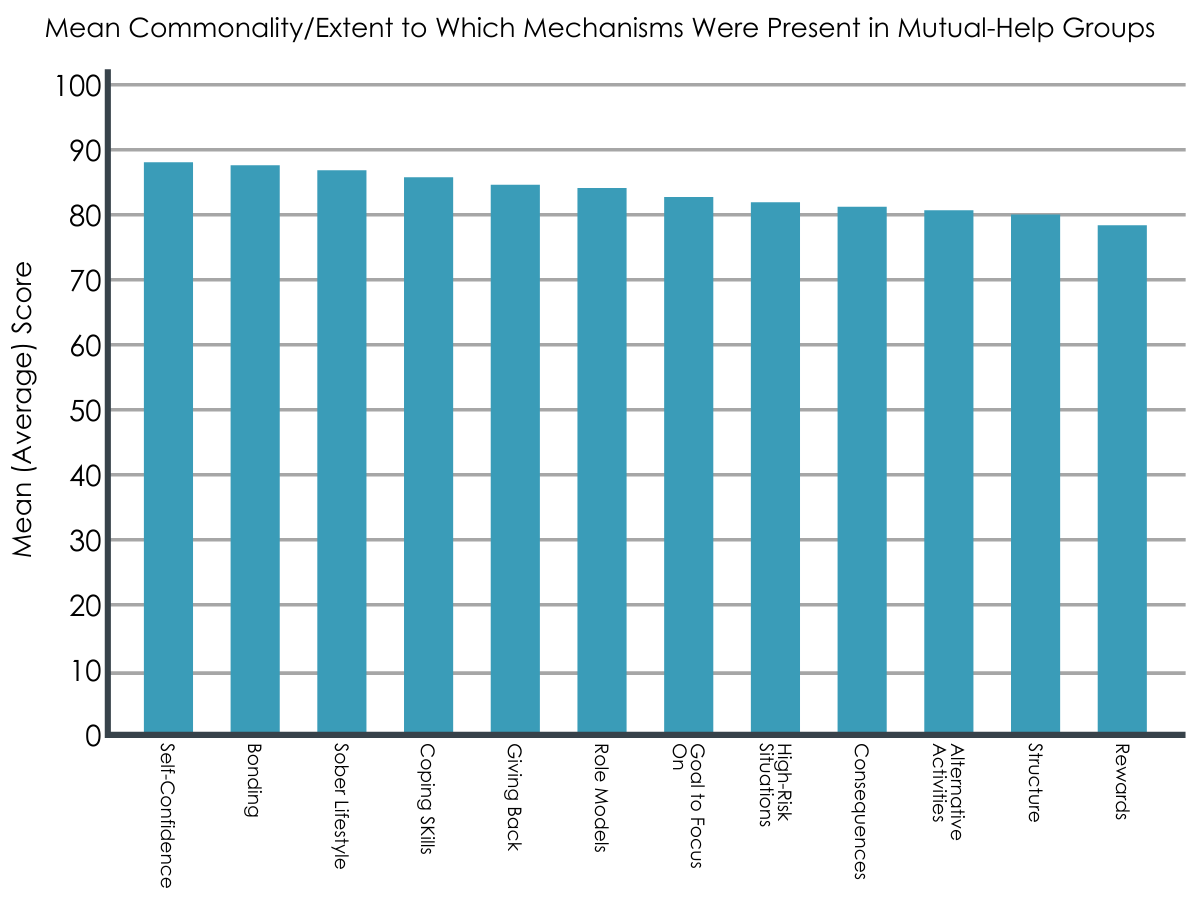
Figure 2.
Mechanisms were identified as equally important among 12-step and non-12-step groups.
The ability to improve confidence was the component ranked as highest in importance, with participants giving it an average score of 90.13 out of 100. Four other potential mechanisms were rated as equally important: developing coping skills; giving back to the community; creating a sober lifestyle; and bonding with others in the group. Notably, these were the same mechanisms that were ranked as most offered. Participants rated the offering of rewards as the least important component, but even it was judged relatively valuable, receiving an average 75.56 out of 100. Participants ranked 5 components as being higher in their significance score than their offered score: goals; structure; giving back; coping skills; and self-confidence. No significant differences appeared in how important these “active ingredients” were among the 12-step, structured non-12-step, and unstructured non-12-step groups. Nor was length of time in recovery associated with the amount of importance attributed to a mechanism of change.

Figure 3.
Descriptions of 12-step and non-12-step groups included the same themes.

Figure 4.
For the qualitative portion of the study, participants were asked to describe their group to a friend or describe a recent experience where the group was helpful. These responses were then analyzed until 5 key themes emerged that were present across the 151 narratives. The themes were perspective taking; being connected to others; developing skills; the value of group activities; and a change in self. Perspective taking: the group allows members to both share their stores and listen to the experiences of others. Participants emphasized that listening to other members describe how they dealt with problems promoted self-awareness and an ability to adopt new perspectives. Being connected to others: participants described the importance of friendship and bonds among group members; being accepted despite their past; stability and safety provided by the group; and the importance of giving and accepting support. Developing skills: whether groups were structured or unstructured, participants emphasized the importance of learning tools that they could transfer to other areas of their lives, including avoiding triggers, setting goals, self-monitoring, and other coping skills. These skills were sometimes associated with increased self-confidence and identified as necessary to maintain permanent change. The value of group activities: some non-12-step groups offered informal activities such as walking, singing in choirs, and making crafts. These activities allowed participants to develop new interests and promoted a sense of achievement. Participants described both 12-step and non-12-step groups as consuming time that was previously dedicated to substance use. A change in self: many participants attributed positive changes in their lives and changes in their sense of self to participation in 12-step groups. They mentioned feeling a new sense of hope that they could change, and that it allowed them to regain their lives.
The research team found that the same themes were present in narratives about 12-step and non-12-step groups. Based on this analysis, they suggest adding two new mechanisms of behavioral change to the preexisting framework employed by the study: “presence of likeminded individuals” and “developing awareness and reflections skills.”
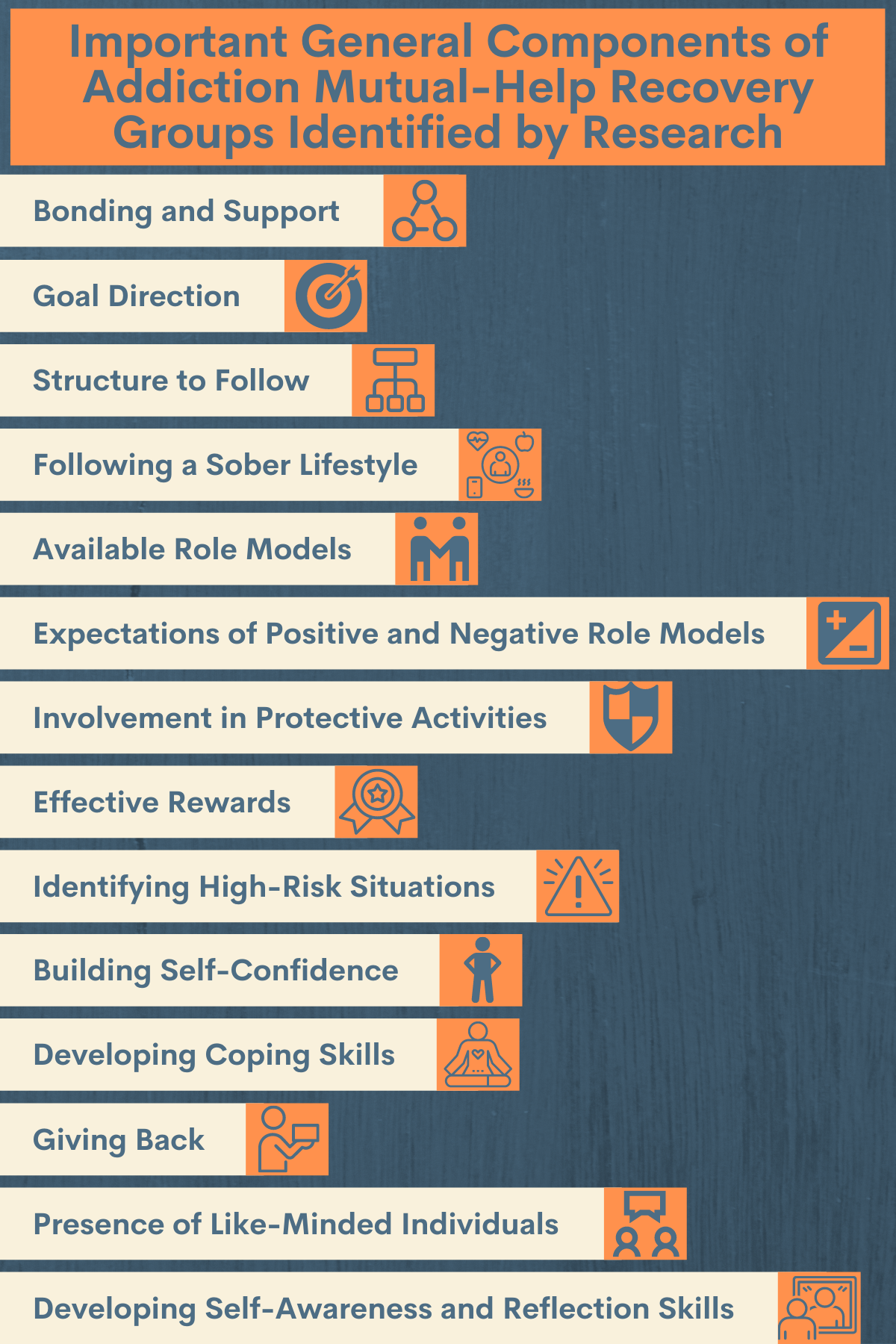
Figure 5.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The effectiveness and cost-effectiveness of AA for alcohol use disorder is strongly supported by multiple experimental studies and some evidence suggests that newer, secular mutual–help organizations such as SMART and Women for Sobriety may be equally effective for those who choose to attend them. This study provides further insight into how people in recovery understand mutual-help’s effectiveness and significant components.
Participants identified all of the potential mechanisms drawn from earlier research as important. On average, they saw their group’s ability to increase self-esteem as most important for their recovery. They ranked the provision of rewards as least important, although participants still ranked it highly. The fact that participants gave all 12 “active ingredients” high scores suggests that they understand their mutual-help group as supporting their recovery in multiple ways, not through a single mechanism. The 5 highest ranked “active ingredients” were also identified as the most offered. They were (in no particular order): building self-confidence; developing coping skills; giving back; bonding with others in the group; and developing a sober lifestyle. This list supports earlier research that suggests social support and creating changes in the social networks of participants is a key “active ingredient” of mutual-help organizations. It also includes elements that highlight the importance of stress and coping (building self-confidence, developing coping skills) as well as behavioral reinforcement/rewards (developing a sober lifestyle). The diversity of these elements reinforces the theory that recovery is a complex process with multiple components that sustain behavior change over time.
This study also suggests that 12-step and non-12-step mutual-help may share many of the same “active ingredients.” The researchers found no significant difference in how offered or how important the components were among 12-step, non-12-step structured, and non-12-step unstructured groups. This finding does not mean that different groups do not have distinct elements that might also attract and support some people’s recovery (such as spirituality or culturally specific components). Nor does it suggest that each group is an equally good fit for every individual. But it does provide some further insight into common mechanisms of behavioral change that people are able to access and mobilize through community-based mutual-help.
This study can help guide further research into which mechanisms of change are most important to which groups of people in recovery; how different mechanisms may interact; and if there are particular aspects of mutual-help groups (for example, group culture or philosophy) that allow individuals to access “active ingredients” in some mutual-help settings and not others. These finding also further support the increased integration of non-12-step mutual-help into contexts such as residential treatment and recovery community centers. Promoting awareness of diverse mutual-help groups through public health messaging can provide more options for people seeking recovery. Promoting LGBQT+ and Black, Indigenous, and People of Color focused recovery groups could also help address the significant gap in culturally appropriate addiction treatment and recovery support at the community level.
- LIMITATIONS
-
- As the authors indicate, this study was based on a convenience sample of people actively involved in recovery groups. Convenience samples are based on people who are easy to access and therefore cannot be assumed to represent an entire group. While informative, the results of this study cannot be generalized to people in recovery more broadly. In particular, these results do not capture people who are unsatisfied with their groups, engage with mutual-help sporadically, or do not attend mutual-help at all. Additionally, this sample was racially homogenous and predominantly male. Future research needs to incorporate greater racial/ethnic and gender diversity—as well as diversity vis-à-vis culture, religion, and sexuality—in evaluating experiences of mutual-help groups.
- The researchers do not provide information about which non-12-step mutual-help groups were included. Nor do they describe the range and kind of unstructured local groups captured by this study. It is therefore difficult to evaluate how well this study captures the full range of non-12-step groups. The similarities between groups described by this study could reflect common mechanisms of change across recovery experiences. But these similarities could also reflect the influence of 12-step mutual-help on other groups, or common influence by a third factor. Further research is necessary to understand how much the mechanisms of recovery supported by mutual-help overlap with other recovery pathways, how much they diverge, and why.
- The mechanisms of behavioral change described in this study potentially overlap in a number of ways. For example, the phrases “sober lifestyle,” “bonding,” “alternative activities,” and “rewards” may be capturing aspects of the same mechanism rather than distinct “active ingredients.” As such, the rating of their importance and presence may not be independent. More granular empirical work can help to determine whether the mechanisms of change derived from existing models adequately capture distinct mechanisms as they operate in mutual-help groups.
BOTTOM LINE
Mutual-help groups are a widely available, community-based, and cost-efficient form of recovery support. Multiple studies underline the effectiveness of Alcoholics Anonymous for supporting recovery from alcohol use disorders. Newer research suggests that other mutual-help groups, such as SMART Recovery and Women for Sobriety, may be as effective for those who choose to attend them. In this study, a group of individuals in recovery identified the same useful elements of participation in 12-step and non-12-step programs. They also identified these elements as equally available across mutual-help groups. Promoting non-12-step mutual-help groups in residential treatment and through recovery community centers could provide more helpful and effective options for individuals seeking recovery, although more research is needed to confirm this and to understand more fully who may benefit more particular mutual-help approaches (e.g., women only groups such as in Women for Sobriety).
- For individuals and families seeking recovery: Today, there are an increasing number of alternatives to traditional 12-step fellowships and initial evidence suggests that they could be as effective as AA for those who choose them. People in recovery have identified several aspects of these groups as important, including building self-confidence; developing coping skills; giving back; bonding with others in the group; and developing a sober lifestyle. Greater levels of active involvement with groups likely produce better recovery outcomes. When evaluating a new recovery support group, people in recovery might ask if these components are present. Service (“giving back”), working with a sponsor/mentor, or socializing with group members each may contribute to getting the most out of mutual-help fellowships.
- For treatment professionals and treatment systems: Multiple studies establish that AA is as effective, and 12-step Facilitation may be more effective, than other psychosocial interventions for alcohol use disorder such as CBT on abstinence outcomes. However, there are legitimate reasons (including family experiences; histories of religious-based trauma; cultural appropriateness) why 12-step programs might not feel safe or welcoming to some people in early recovery. For people who are unable to engage with 12-step fellowships, groups such as SMART and Women for Recovery represent alternatives and appear to incorporate many of the same kinds of therapeutic elements found in AA or NA.
- For scientists: This study illustrates the benefits of incorporating perspectives of people in recovery into research on recovery supports. While existing research establishes the effectiveness of AA, this article suggests that the some of the same mechanisms of change can be found in both 12-step and non-12-step groups. Further research is necessary to understand whether additional mechanisms are present in some groups and not others, and whether some aspects of mutual-help groups (e.g., gender-specificity, group culture or philosophy) allow particular groups to engage with these processes while preventing or excluding others. Additionally, the fact that participants pointed to different kinds of “active ingredients” (social learning; social reinforcement; behavioral modification; stress coping) reinforces the understanding that recovery is a complex process with multiple, interacting mechanisms. Theories and models of recovery should reflect this complexity.
- For policy makers: Research has established that community-based recovery groups are an effective and highly cost-efficient means of supporting recovery from SUDs. Traditionally, these groups have been identified with 12-step programs such as AA or NA. Recent studies suggests that newer mutual-help groups—such as SMART, LifeRing, Recovery Dharma, All-Recovery Meetings, and Women for Recovery—may be helpful for those choosing to attend them. The existence of these alternative fellowships is still little known. Incorporating links to these groups into public health information and campaigns may be beneficial, especially for individuals who do not wish to engage in 12-step fellowships. Funding recovery community centers can help make these newer fellowships more readily accessible, providing new entry ways into recovery. Promoting LGBQT+ and Black, Indigenous, and People of Color focused recovery groups could also help address the significant gap in culturally appropriate addiction treatment and recovery support at the community level.
CITATIONS
Rettie, H. C., Hogan, L. M., & Cox, W. M. (2021). Identifying the main components of substance-related addiction recovery groups. Substance Use and Misuse, 56(6), 840–847. DOI: 10.1080/10826084.2021.1899228